
988
Convening Playbook
Lifeline Contact Centers
1
Acknowledgements
Many organizations contributed their time and expertise to the development of this
document, including:
988 Collaborative of Crisis Centers
American Association of Suicidology
Arizona Complete Health
Arizona Health Care Cost Containment System (AHCCCS)
Behavioral Health Response (Missouri)
Crisis Text Line
Didi Hirsch (California)
Guam Behavioral Health & Wellness Center
Integral Care (Texas)
International Council of Helplines
Lines for Life (Oregon)
McKinsey Health Institute
National Alliance on Mental Illness (NAMI)
National Association of Crisis Center Directors (NASCOD)
National Coalition for Mental Health Recovery (NCMHR)
National Council for Mental Wellbeing
National Emergency Number Association (NENA)
National Empowerment Center (NEC)
On Our Own of Maryland
People-USA (New York)
Solari (Arizona)
The Harris Center for Mental Health and Intellectual and
Developmental Disabilities (Texas)
Trevor Project
Vibrant Emotional Health
Volunteer of America Western Washington (VOAWW)
2

988 Convening Playbook
Lifeline Contact Centers
Overview
Goal: The
document sets out to help:
• Articulate the need for operational readiness for 988
• Help Lifeline contact centers prepare for the 988 transition (not a specific mandate for
them)
• Explain how to make progress on the criteria that are central to 988 readiness
• Identify best practices and examples seen in the field today
Audience: This document is intended for the directors and leaders of Lifeline contact centers
Structure: The document has three sections:
I. Operational readiness self-as
sessment
II. Playbook
III. Additional resources
Not
es:
• Equity: The playbook aims to highlight equity considerations across topics, including
how equity needs to be considered across all areas of readiness
• Case studies and examples: The pl
aybook includes many case studies and examples
from individual lifeline contact centers. Examples will not be applicable to all Lifeline
contact centers
• Resources: The pl
aybook includes links to the National Suicide Prevention Lifeline’s
Net
work Resource Center
(NRC), a resource specifically for Lifeline contact centers
(
https://networkresourcecenter.org/plugins/servlet/samlsso?redirectTo=%2Fhomepag
e.ac
tion).
1
1
Access to the NRC is for Lifeline contact centers and can be set up by the Lifeline administrator.
3
Table of Contents
I. 988 operational readiness self-assessment for Lifeline contact centers ........ 5
Introduction and purpose of the operational readiness self-assessment ................... 5
Self-assessment levels .............................................................................................. 5
Link to playbooks ....................................................................................................... 5
Criteria ...................................................................................................................... 6
II. Playbook for Lifeline contact centers .............................................................. 15
1. Workforce .......................................................................................................... 15
Workforce management strategy and systems ........................................................ 15
Addressing staffing needs through hiring and retention ........................................... 22
2. Financial sustainability ..................................................................................... 32
Resources to identify potential sources of ongoing funding and build diverse funding
sources ................................................................................................................... 33
Improving insurance billing capabilities and related considerations ......................... 34
3. Connection to 911 / PSAPs ............................................................................... 36
Process to develop relationships with PSAPs .......................................................... 36
Transfer of calls from 911 to 988 ............................................................................. 37
Transfer of calls from 988 to 911 ............................................................................. 37
Data-sharing approach ............................................................................................ 38
Systems and interoperability .................................................................................... 39
Universal and convenient access ............................................................................ 42
High quality and personalized experience ............................................................... 44
Connection to local resources and follow-up ........................................................... 46
III. Additional resources ........................................................................................ 50
IV. Appendix .......................................................................................................... 52
Appendix A: Active surge management example protocol from BHR ....................... 52
Appendix B: MOUs between contact centers and PSAPs ........................................ 53
Appendix C: LAPD 911 dispatch protocol for diverting calls involving persons
experiencing a mental health crisis to Didi Hirsch .................................................... 56
Appendix D: LAPD 911 diversion guide for crisis counselors and supervisors ......... 58
4

I. 988 operational readiness
self-assessment for Lifeline contact
centers
Introduction and purpose of the operational readiness
self-assessment
The s
elf-assessment tool is intended to assist Lifeline contact centers (“centers”) in
assessing their readiness for the July 2022 transition to 988 and prioritizing areas of focus
moving forward.
The tool is not i
ntended to be evaluative, and no responses will be collected or aggregated.
There is neither a perfect score nor
a right answer. The intent is solely to help Lifeline contact
centers determine where they might focus efforts both ahead of July 2022 and beyond as the
country moves toward integrated crisis care.
In addition, there is no time expectation associated with the self-assessment tool. Lifeline
contact centers are working in different contexts and all have different priorities and needs
related to 988 and integrated crisis care. The goal of this self-assessment tool is to help
Lifeline contact centers define an aspiration unique to their locality, not prescribe any
activities on a specific timeline.
Self-assessment levels
The s
elf-assessment tool lays out a series of criteria within specific readiness categories that
are aimed at holistically capturing components of readiness to realize the full potential of 988.
For each criterion, centers can select from three distinct levels. Lifeline contact centers are
asked to select the level that best approximates their current state.
• Beginning: Work in this area has not yet started
• Emerging: Work in this area is underway but not yet complete
• Solidified: Objectives in this area are fully or almost fully met
Some criteria reference specific services that may not be applicable to every organization.
E
ach organization can choose to focus on the criteria that are most relevant for it.
Link to playbooks
The s
elf-assessment categories match categories of information contained in the rest of the
playbook document. The results of the self-assessment can be used to determine on which
areas of the playbook centers should consider focusing in the immediate term.
5

For example, Lifeline contact centers who are “beginning” work within specific categories that
they believe are important can use information from the playbook to chart a path to initiate
activities aimed at achieving “emerging” readiness. Centers that are already “emerging” in
certain categories can use the playbook to fully solidify their readiness in those categories.
Criteria
Criteria
Beginning
Emerging
Solidified
UNIVERSAL AND CONVENIENT ACCESS
Reliable and timely response: All persons contacting 988 will be connected to professionally
trained individuals reliably, efficiently, and in a timely manner.
How timely and efficient
is the response to Lifeline
calls?
80 percent
answered in 60
seconds or lower
service level (e.g.
,
<80 percent, >60
seconds)
90 percent answered
in 60 seconds
90 percent answered
in 15 seconds
What share (%) of Lifeline
calls are currently
answered?
Less than 70
percent of Lifeline
calls are answered
70-90 percent of
Lifeline calls are
answered
More than 90 percent
of Lifeline calls are
answered
How does the center’s
timeliness and efficiency
of response on the
Lifeline compare to its
other lines of business
(LOBs), particularly those
that are well-funded, if
applicable?
Less timely and
efficient response
compared to other
lines of business
Equally timely and
efficient response
compared to other
lines of business
Multi-channel availability: 988 will be accessible through various modalities based on individuals’
needs and routed to network centers via a central administrator
More timely and
efficient response
compared to other
lines of business
To what extent does the
center provide coverage
for Lifeline calls?
Does not provide
coverage for
Lifeline calls
Provides some, but
not 24/7 coverage for
Lifeline calls
Provides 24/7
coverage for Lifeline
calls
To what extent does the
center provide any
coverage for non-
Lifeline texts?
Does not provide
coverage for texts
Provides some, but
not 24/7 coverage for
texts
Provides 24/7
coverage for texts
To what extent does the
contact center provide any
coverage for non-
Lifeline chats?
Does not provide
coverage for chats
Provides some, but
not 24/7 coverage for
chats
Provides 24/7
coverage for chats
6

Criteria
Beginning
Emerging
Solidified
HIGH QUALITY AND PERSONALIZED EXPERIENCE
Tailored support: 988 will be a source of personalized, trusted support (e.g., tailored support for
familiar callers, specialized services to meet functional, linguistic, or cultural needs)
To what extent does the
center provide and link
individuals to services
that are person-centered
(culturally appropriate,
linguistically appropriate,
inclusive of support
systems, etc.)?
No person-
centered services
or links to person-
centered services
are provided
Some person-centered
services and/or links to
person-centered
part
ners are provided,
but it is not 24/7 and/or
onl
y for a limited set of
populations
Person-centered
services and links to
person-centered
part
ners (including
spec
ialized services,
warmlines, and pe
er-
run resources) are
pr
ovided 24/7 for a
comprehensive set of
populations
To what extent does the
contact center have
training to provide
services that are person-
centered (culturally
appropriate, linguistically
appropriate, inclusive of
support systems, etc.) for
groups with unique needs
and/or at higher risk for
suicide?
2
No training to
provide person-
centered services
or on how to
identify links to
specialty partners
Some training to
provide person-
centered services
and/or identify links to
specialty partners but
only for a limited set of
populations
Training to provide
person-centered
services and links to
specialty partners
(including warmlines
and peer-run
res
ources) are
prov
ided 24/7 for a
comprehensive set of
populations
How are familiar
contacts identified and
effectively served (e.g.,
ensuring that counselors
are providing connections
to long-term support when
appropriate)?
No process in place
to identify and
provide specific
assistance to
familiar contacts
Familiar contacts are
identified informally
and plans for assisting
and care coordination
are prepared on an
ad-hoc basis
Familiar contacts are
identified through a
formal process, and
there is a standard
procedure in place to
review their needs and
alert crisis counselors
on how to best assist
them, including
collaborating on care
coordination plans
How are counselors
trained to identify and
effectively serve familiar
contacts (e.g., ensuring
that counselors are
providing connections to
long-term support when
appropriate)?
Crisis counselors
do not receive
training on best
practices in working
with familiar
contacts
Crisis counselors
receive informal
training on best
practices in working
with familiar contacts
All crisis counselors
receive formal training
on best practices in
working with familiar
contacts
2
SAMHSA notes people at greater risk for suicide include but are not limited to: adults over the age of 45, American Indians,
Alaskan Natives, veterans, LGBTQ+, youth and young adults, attempt survivors, loss survivors, and disaster survivors.
Source: “People at greater risk of suicide,” Substance Abuse and Mental Health Services Administration,
https://www.samhsa.gov/suicide/at-risk; The National Suicide Hotline Designation Act of 2020 describes this group as “LGBTQ
youth, minorities, rural individuals, and other high-risk populations,” Source: “Text – S.2661 – 116
th
Congress (2019-2020):
National suicide hotline designation act of 2020,” Congress.gov, October 17, 2020, https://www.congress.gov/bill/116th-
congress/senate-bill/2661/text.
7

Criteria
Beginning
Emerging
Solidified
To what extent does the
center have a relationship
with Tribal reservation(s)
in the catchment area, as
relevant?
Does not have any
formal relationship
or processes in
place to identify
and respond to
Tribal needs
Has informal
relationships and
some processes in
place to respond to
T
ribal needs (e.g.,
identifying individuals
living on Tribal
reservations, ability to
connect individuals to
Tribal resources for
further support)
Has formal
relationships and
processes in place to
identify Tribal contacts
and route individuals
to the appropriate
Tribe's systems /
services (e.g., Bureau
of Indian Affairs vs.
law enforcement,
Tribe vs. State-run
medical facility)
Consistency in line with best practices: All persons contacting 988 should receive care in line
with best practices.
How is the risk of suicide
assessed?
Center uses suicide
assessment tool
that no longer
meets Lifeline 2007
assessment
standards or does
not consistently use
a compliant tool
Center uses suicide
assessment tool that
meets Lifeline 2007
assessment standards
Center uses suicide
assessment tool that
has been updated to
reflect the Lifeline
Safety Assessment
(2018)
How does the center
address safety planning?
Center does not
use a safety
planning process
with callers /
chatters / t
exters or
provide training to
crisis counselors on
effective de-
escalation and
safety planning
Center uses an
informal safety
planning process with
callers / c
hatters /
texters and provides
some training to crisis
counselors on
effective de-esc
alation
and safety planning
Center uses a formal
safety planning
process with callers /
chatters / t
exters and
provides extensive
training to crisis
counselors on
effective de-esc
alation
and safety planning
Does the center have
required policies in place
addressing Lifeline
contacts at imminent risk
of suicide?
Center has policies
in place that no
longer meet Lifeline
imminent risk
requirements or
does not
consistently train in
or use these
policies
Center has policies in
place that meet some
but not all Lifeline
imminent risk
requirements and
consistently t
rains in
and uses these
policies
Center has policies in
place that meet all of
the Lifeline imminent
risk requirements and
consistently trains in
and uses these
policies
8

Criteria
Beginning
Emerging
Solidified
How is workforce (e.g.,
crisis counselors,
volunteers) training
conducted to ensure best
quality service?
Lifeline-endorsed training
includes the Safety
Assessment site,
simulation trainings, the QI
monitoring instrument,
ASIST, Lifeline training
modules, and NRC tools.
No formal training
in place
OR
Some formal crisis
counselor training
occurs, but does
not inc
orporate any
Lifeline-e
ndorsed
or developed
training tools for
staff responding to
Lifeline contacts
Some formal crisis
counselor training
occurs. Training
incorporates some
Lifeline-e
ndorsed or
developed training
tools for staff
responding to Lifeline
contacts
Extensive curriculum-
based crisis counselor
training occurs.
Training consistently
incorporates Lifeline-
endorsed or
developed training
tools for staff
responding to Lifeline
contacts
How is workforce (e.g.,
crisis counselors,
volunteers) supervision
conducted to ensure best
quality service?
No formal
supervision is in
place for workforce,
and/or there is
inconsistent access
to a supervisor
during all crisis
counselor shifts
Supervision is
accessible as needed
for all team members,
and a supervisor can
be consulted at
all
times of center
operation
Formal and
consistent supervision
meetings are in place
for all team members,
and a supervisor can
be consulted at
all
times of
center
operation. Team
members have real-
time supervision and
guidance for text
/
chat, as relevant
How are dispatch or
referral decisions (e.g.,
facilitating real time
connections to crisis care)
determined (e.g., whether
to dispatch a crisis mobile
team (CMT) or rescue, to
coordinate facility-based
care or outpatient follow-
up care)?
There is no
consistent
guidance on
dispatch or referral
decisions for
contacts
Some staff may use
an assessment
protocol to determine
dispatch or make
referral decisions, but
the assessment is not
standardized or is not
consistently used
Centers use an
accepted assessment
protocol to determine
dispatch and make
referral decisions
To what extent is there a
defined performance
management strategy
(e.g., key performance
indicators defined, data
collected, data reported,
frequency with which data
is reviewed and acted
on)?
No central
performance
management
strategy
Data is collected
and/or reported, but
does not fit into a
performance
management strategy
Data is collected and
reported against a
defined set of key
performance
indicators (K
PIs) and
discussed and acted
on consistently and at
a regular schedule. A
Continuous Quality
Improvement (CQI)
plan incorporates
insights from data
9

Criteria
Beginning
Emerging
Solidified
To what extent does the
center use the
performance
management strategy to
implement continuous
improvement and ongoing
training programs guided
by data (e.g., silent
monitoring)?
No continuous
improvement or
ongoing training
programs in place
Some data-driven
continuous
improvement and
ongoing training
programs in place
Data-driven
continuous
improvement and
ongoing training
programs are in place
How are local
collaborators (e.g.,
government, public safety,
providers) included in
regular performance
management reviews to
improve systems
efficiencies and
effectiveness?
No arrangements
nor regular
meetings in place
to develop / refin
e
performance
criteria and review
potential systems
improvements
Informal arrangements
in place to develop /
refine performance
criteria and review
potential systems
improvements, but
meetings and
engagement with
essential collaborators
are not consistent or
inclusive of key
stakeholders
Formal arrangements
in place to regularly
develop / refine
perfor
mance criteria to
review potential
systems
improvements, and
meetings and
engagements with
essentia
l stakeholders
are cons
istent and
appropriately inclusive
CONNECTION TO LOCAL RESOURCES AND FOLLOW-UP
Localized response: All persons contacting 988 will be connected to helpline support and
additional local community resources as needed.
What is the center's
relationship with local
mobile crisis teams
(MCTs), if available?
Does not have a
relationship with
local MCTs
Has an informal
relationship with local
MCTs which enables it
to mak
e referrals to
their services, but no
formal agreement
Has a memo of
understanding (or
contract) with local
MCTs or directly
operat
es a CMT,
enabling efficient
referrals and
exchange of
information between
services
What is the contact
center's relationship with
CSRFs, if available?
Does not have a
relationship with
local CSRFs
Has an informal
relationship with local
CSRFs and can make
ref
errals, but no formal
agreement
Has a memo of
understanding with
local CSRFs or
di
rectly operates a
crisis receiving and
stabilization facility,
enabling efficient
referrals and
exchange of
information between
services
10

Criteria
Beginning
Emerging
Solidified
What is the process to
coordinate facility-based
crisis care?
No process in place
to connect
individuals to
facility-b
ased crisis
care
A database or list of
local facility-based
crisis care referrals
exists, but
coordination is limited
to referral (e.g., no
warm handoff or
coordination with
facility)
A database or list of
local facility-based
crisis care ref
errals
exists and
coordination with
facilities occurs
through warm
handoffs and/or direct
coordination with
facilities
Connection to local public health and safety services: 988 can connect to local public health
and safety services to provide appropriate support while avoiding unnecessary law enforcement
involvement, emergency department use, and hospitalization.
What is the contact
center's relationship with
local 911 / Public Safety
Answering Points
(PSAPs), potentially
including local ambulance
and emergency medical
services (EMS)?
Does not have a
relationship with
local 911 / PS
APs
and local
ambulances /
EMS
Has an informal
relationship with local
911 / P
SAPs and local
ambulances /
EMS but
no formal agreement
Has a memo of
understanding with
local 911 / PS
APs or
works
directly within
911 / P
SAPs as well
as local ambulances /
EMS for relevant
services, enabling
efficient referrals and
exchange of
information between
services
What is the process to
receive contacts from
local 911 / PSAPs?
No process in place
given lack of formal
agreement and/or
technology
capabilities
No process in place,
but both PSAP entities
and the center ar
e
interested in
transferring 911
mental health (MH)
contacts; ho
wever,
they lack resources,
technologies, or other
capabilities
Process in place to
receive MH crisis calls
from 911
What is the contact
center's relationship with
local emergency
departments?
Does not have a
relationship with
local emergency
departments
Has an informal
relationship with local
emergency
departments but no
formal agreement that
enables exchange of
information between
services
Has a memo of
understanding with
local emergency
departments or works
directly within local
emergency
departments, enabling
efficient exchange of
information between
services
11

Criteria
Beginning
Emerging
Solidified
What is the contact
center's relationship with
local information and
referral services (e.g.,
211)?
Does not have a
relationship with
local information
and ref
erral
services
Has an informal
relationship with local
information and
referral services but no
formal agreement
Has a memo of
understanding with
local information and
referral services or
works directly with
i
nformation and
referral services (e.g.,
co-located with or ru
ns
211)
Defined process in
place to receive MH
crisis contacts from
local information and
referral services (e.g.,
warm transfer
services, information
sharing, follow up
contacts
)
Follow-up as needed: As appropriate, persons contacting 988 may be offered follow-up services to
facilitate on-going support and safety.
How is crisis follow-up
conducted?
Does not provide
crisis follow-up
services
Sometimes provides
crisis follow-up
services on an ad-hoc
bas
is but lacks
standard protocols
Crisis follow-up
services are provided
according to standard
protocols
What is the process to
coordinate outpatient
follow-up care?
No process in place
to connect
individuals to
outpatient follow-up
car
e
A database or list of
local outpatient care
exists, but
coordination is limited
to referrals (e.
g., no
warm handoff or
appointment
scheduling)
A database or list of
local outpatient care
referrals exists, and
care coordination
occurs through warm
handoffs and/or
appointment
scheduling
FUNCTIONAL ENABLERS
WORKFORCE
What is the ability to
monitor and optimize
efficiencies in staffing
needs to meet 988
demand?
Center does not
currently have a
workforce
management
system that can
effi
ciently
determine trends in
service demands
per shift
Center has a
workforce
management system
(automated or manual)
that helps determine
trends in service
demands per shift,
though it still has gaps
in st
affing optimization
Center has an
automated workforce
management system
that can efficiently
determine service
demands per shift
12

Criteria
Beginning
Emerging
Solidified
If hiring is identified as a
challenge, what capability
does the center have to
hire staff for in person,
telework, or remote (non-
geographically limited)
roles?
Center hires staff
only or mostly only
from the immediate
community for in-
person work. No
significant telework
/ virtual roles
available
Center hires staff
mostly from the
immediate community,
but offers some limited
telework and virtual
roles
Center hires staff from
the immediate
community and is able
to hire people across
the state and country.
Center supports virtual
and teleworking roles
as appropriate
How does the center
staffing (i.e., both paid
and volunteer team
members) align to
service demand /
response needs?
Center frequently
struggles to identify
and hire the staff
needed to respo
nd
to demand
Center generally has
sufficient staffing but
may have trouble
identifying and hiring
new staff as demand
increases
Center continuously
has sufficient staffing
and can easily identify
and hire new staff as
demand increases
FINANCIAL SUSTAINABILITY
To what extent has the
cost of 988
implementation at the
center (e.g., facilities
costs, technology, staffing,
administrative costs) been
estimated and budgeted
for?
The cost of 988
implementation has
not been estimated
or budgeted for
The cost of 988
implementation has
been estimated but not
budgeted for
The cost of 988
implementation has
been estimated and
budgeted for
To what degree is the
current funding strategy
sufficient for ongoing
center operating costs?
Ongoing funding is
insufficient to cover
all center operatin
g
costs
Funding is in place to
support short-term
operations (<2 years),
and consider
s
Vibrant's expectations
for the cost of 988
implementation (start-
up costs)
Funding is in place to
support longer-term
operations (>2 years)
and considers
Vibrant's expectations
for the cost of 988
implementation (start-
up costs)
How does the center
receive ongoing
funding?
Ongoing funding is
currently received
from a single
source
Ongoing funding is
currently received
through several
sources, but is not
predictable in the long-
term
Ongoing funding is
currently received
from multiple,
sustainable sources
with recurring
availability
TECHNOLOGY & DATA
To what extent is the
center’s local 988 contact
documentation system
coordinated with the
national 988 data-
reporting needs?
Local contact
documentation
system is not
readily capable of
collecting and
reporting the
minimally required
988 data to the
Lifeline (as per the
Network
Agreement)
Local contact
documentation system
is readily capable of
collecting and
reporting the minimally
required 988 data to
the Lifeline, but it does
not us
e standardized
data elements for
Lifeline contacts
Local contact
documentation system
for 988 uses
standardized data
elements for Lifeline
contacts
13

Criteria
Beginning
Emerging
Solidified
To what extent is
Automatic Call
Distribution (ACD)
functionality implemented?
No ACD
functionality
incorporated
Limited functionality
and/or plan to develop
ACD functionality
ACD functionality
incorporated
To what extent is Caller ID
functionality
implemented?
No Caller ID
functionality
incorporated
Limited functionality
and/or plan to develop
Caller ID functionality
Ability to ID every call
received by call center
How are contact
summary data (e.g., user
inputs) shared with
partners (e.g., 911 or other
transport service, MCT,
emergency departments
or other receiving facilities,
treatment facilities)?
Staff cannot send
summary data to all
partners, and there
is not a plan to
create this
capability
Staff cannot send
summary data to all
partners, and there is
a plan to create this
capability
Staff can send
summary data to all
partners
How are contact
metadata (e.g., caller ID,
address, IP address)
shared with partners (e.g.,
911, MCT, treatment
facilities, other transport
services)?
Staff cannot send
metadata to all
partners, and there
is not a plan to
create this
capability
Staff cannot send
metadata to all
partners, and there is
a plan to create this
capability
Staff can send
metadata to all
partners
How does the center track
and project contact
volumes and
performance metrics?
No or limited ability
to project or track
contact volumes
consistently across
all channels (e.g.,
call, text, chat)
Contact volumes are
projected and tracked
across all channels
(e.g., call, text, chat)
through manual
processes such as
spreadsheets
Contact volumes are
projected and tracked
across all channels
(e.g., call, text, chat)
with forecasting
sof
tware
14

II. Playbook for Lifeline contact
centers
1. Workforce
Lif
eline contact centers already face unique challenges related to workforce hiring,
management, and retention. Optimizing the workforce will become even more critical with the
expected volume increases associated with the 988 transition. The following section
highlights potential approaches for contact centers to (1) accurately determine their staffing
needs by using workforce management, and (2) address these needs through both hiring
and retention.
Before implementing a workforce management strategy to determine how to optimize their
use of their workforce, it is important for centers to accurately determine their staffing needs.
To best determine these, a center can consider its staffing model (both the number of
individuals needed and their distribution across functions) in the context of its service level
goals. Centers can then evaluate their staffing model by looking at the number of team
members per function to determine if the current distribution of team members supports the
service level goals. For instance, they could assess the current balance between team
members that answer contacts (e.g., counselors) and other team members (e.g., support,
scheduling, training).
Embedding cultural and linguistic competencies is also critical in building and modifying a
center’s staffing model so it can best serve the community.
Additional information: Cultural and linguistic competency, including information about the
National Standards for Culturally and Linguistically Appropriate Services (CLAS) and free
accredited online educational programs, is provided by the Office of Minority Health
(https://minorityhealth.hhs.gov/omh/browse.aspx?lvl=1&lvlid=6).
3
Workforce management strategy and systems
Wor
kforce management strategy
Lifeline contact centers can implement a workforce management strategy that efficiently
identifies trends in service demands at a per-shift level.
Key steps in workforce management are described by Vibrant Emotional Health, the current
operator of the National Suicide Prevention Lifeline (NSPL). They include:
4
• Forecast call volume (or “traffic load”) for multiple 15- to 30-minute intervals
• Determine staffing levels for each interval (number and types of agents)
3
“Cultural and linguistic competency: National CLAS standards,” U.S. Department of Health and Human Services, Office of
Minority Health, last modified December 30, 2021, accessed February 7, 2022,
https://minorityhealth.hhs.gov/omh/browse.aspx?lvl=1&lvlid=6.
4
National Suicide Prevention Lifeline, Vibrant Emotional Health, and Substance Abuse and Mental Health Services
Administration, “Crisis call center metrics: Part 1. Service and efficiency,” accessed Feb. 7, 2022,
https://suicidepreventionlifeline.org/wp-content/uploads/2019/02/CallCenterMetrics_final.pdf.
15

• Schedule call center agents
• Monitor and manage performance in real time, as needs fluctuate
• Evaluate strategy by asking questions such as:
o Is the software functionality adequate?
o Were shifts covered?
o Were per
formance measures met?
o Are there any interesting trends in call volume data?
Workf
orce management (WFM) systems
5
Wor
kforce management systems support the effective implementation of workforce
management strategies. Workforce management systems generally:
• Support forecasting, monitor performance, and m
anage day-to-day assignments and
scheduling
• Operate in an automated wa
y
• Work with existing call center systems
• Support the handl
ing of surge capacity
An ideal
workforce management system would include scheduling, real-time adherence,
reporting, and data collection, and would communicate in a clear, concise manner. Real-time
monitoring is an important part of any workforce management system, as it will ensure
coverage is maintained and key performance indicators are being met within each center.
Additionally, it helps maintain schedule adherence and efficiently monitors operational
issues.
The process of setting up a new workforce management system is often initiated by the
product team in the beginning of the process and completed by the call center team, which
uses their specific data, goals, and needs. To set up a system, the teams would enter the call
center’s metric goals, employee data, schedules, hours of operation, and site locations if
needed. Setup would also include entering the forecasts, average handle times, and
shrinkage data; this will help facilitate the system’s forecasting ability going forward.
Example workforce management systems include but are not limited to:
• Verint Monet
WFM
: Capable of handling day-to-day basic workforce management
(https://www.verint.com/grow-my-smb-bu
siness/)
• Alvaria workforce management
: Has additional, optional capabilities
(https://www.alvaria.com/landing-pages-2021/
call-center-wfm-software-
2022?gclid=EAIaIQobChMIzvrEhoGK9gIVFmxvBB32oADxEAAYASAAEgLd2vD_Bw
E)
5
Bart Andrews, Vice President of Clinical Practice / Evaluation at Behavioral Health Response, February 2022.
16

Case study: Behavioral Health Response (BHR)
(Missouri)
6
BHR uses the Verint Monet WFM system, which includes a real-time monitoring
dashboard and scheduling views. The monitoring dashboard shows information at the
center and employee activity le
vels, including each employee’s status (e.g., answering
calls, wrapping, taking a break) and upcoming schedule, while the scheduling views
enable the user to see shift coverage at the daily level. The system allows the center to
see customized reports and statuses as well.
BHR’s real-
time monitoring dashboard:
BHR’s schedule dashboard:
6
Bart Andrews, Vice President of Clinical Practice / Evaluation at Behavioral Health Response, February 2022.
17

Center-specific information:
Surge Capacity: BHR created and maintains a detailed surge plan to address both
planned and unplanned call volume increases, which it is able to monitor real-t
ime using
Verint Monet WFM. BHR receives automated alerts based on wait times and pushes
notifications to staff when call volume exceeds certain parameters. Cent
ers hold regular
meetings with key staff to review performance metrics, staffing levels, call volume levels
and projections of volume levels based on new information or planned events. Teamwork
and agreed-upon ex
pectations are key to managing call volume and supporting staff
during call surges.
If BHR anticipates call volume surges (for example, due to site closure, agency phone
problems), it
can request extra staffing in advance.
BHR’s Operations Analyst sends out a
reminder on days where additional coverage for
the agenc
y’s phones is necessary and reminds the center’s staff when to be especially
conscious of their Do Not Disturb (DND) use. BHR’s Active Surge Management protocol is
detailed in the A
ppendix.
18

Case study: Lines for Life (LFL) (Oregon)
7
According to LFL, an ideal workforce management system:
•
Allows staff to clock in and out through the phone system so that supervisors can
see when colleagues are present
• C
ontains in-house training and emergency contact information
• Houses the call-takers’ schedules and PTO calendars
•
Keeps track of how much time off staff are taking
• Includes its own texting platform
• Offers an internal chat system to enable communications
• Includes an agent status dashboard, scheduling database, and center workforce
overview
A
gent status board: Th
e agent
status boards allow supervisors to see the real-time
status of each crisis intervention specialist
Scheduling database: LFL uses Better Impact as its scheduling database. It contains the
profiles of all call-ta
king staff. It also houses the training modules, surveys, contact
information, and allows LFL to send texts to all staff.
7
Dwight Holton, CEO of Lines for Life.
19

Telephony dashboard: The telephony dashboard allows LFL to see how much of the
workforce is available at
the moment. It also shows how many callers are waiting and
daily performance.
20

Surge Capacity: LFL crisis workers who have met high standards for quality, attendance,
and reliability are invited to become part of a back-up team. As a back-up team
member, the
y agree to receive text notifications when there is need for additional
coverage on t
he crisis lines. Back-up mem
bers who sign up to cover a back-up team shift
receive a higher hourly wage for those shifts, with
an additional differential added for
swing shifts, overnight s
hifts, and weekend shifts. LFL sends out a group text to the back-
up team when it is alerted to the possibility of a sudden / temporar
y spike in call volume.
With the Veterans Crisis Line (VCL) contract, LFL has had good success with offering pay
incentives for staff to cover the lines for an anticipated or unexpected surge in call
volume. For
example, in 2021, VCL gave LFL advance notice of a four- to six-hour shut-
down for maintenance on seven occasions. For the most recent shutdown in 2021, LFL
was able to recruit a team of 30 crisis intervention specialists, supervisors, team leads and
directors who worked from 8:30 PM until midnight to cover the shutdown. This team
successfully answered 122 calls in three hours—79 on the VCL and 43 on the other line—
compared with typical volumes of 70-100 calls over a 12-hour period on VCL.
Case study: Solari (Arizona)
8
Solari has taken multiple steps to adopt the following practices to build surge capacity into
workforce planning. Solari found that maintaining adequate staffing on 24/7 lines required
the ability to manage sudden or prolonged increases in overall call volume. The four
components of surge capacity Solari identified are structure, staff, stuff, and systems.
During the pandemic, needs across all four of these areas were determined to be critical
to manage surge capacity:
1. Ability to socially distance (structure)
2. Contact center and dispatch team members (staff)
3. Sanitizing and cleaning supplies (stuff)
4. Efficient, nimble electronic health records (EHR) that
can be utilized regardless of
locati
on / system
S
olari has procedures to accommodate call surges and regularly receives
communi
cations from NSPL about certain television interviews, tragedies, social media,
and other events that may increase call volume. Solari also answers the Tragedy Support
Line, which frequently experiences increased v
olume after a local distressing event. It has
a blended workforce of on-site and remote staff, with on-call staff that can assist during a
surge and be activated quickly.
To address the issues surrounding structure, Solari made the decision to offer and/or
transition staff members to remote / h
ome-based response and create a small onsite
team for both continuity planning and supervisory oversight. This allowed it to place team
members in their own offices, which lessened contact and maximized social distancing. It
also ensured that engagement with staff was frequent, and that leadership was present
24/7 for the first few months. This allowed flexible coverage when staff members had to
call out. The facilities team was very proactive in securing sanitization supplies from
vendors and the EHR was configured so location was not a barrier to access. Solari did
have to provide additional IT support to team members when they initially went remote,
8
Justin Chase, President and CEO of Solari Crisis and Human Services.
21

but it was able to quickly dial back the amount of support needed. This was mostly due to
the high level of technical training that had been provided to center leadership.
Additi
onal information: How to forecast volume and determining staffing needs using
Erlang modeling can be found in Vibrant’s Crisis Call Center Metrics
guide
(https://suicidepreventionlifeline.org/wp-
c
ontent/
uploads/2019/02/CallCenterMetrics_final.pdf).
9
Addressing staffing needs through hiring and retention
Ensuri
ng appropriate staffing levels requires focusing on talent recruitment, retention, and
organizational health, as well as tools and standards for learning and development. The
following section outlines potential levers to support both hiring and retention.
The first step will be to define goals for talent recruitment, retention, and organizational
health along with timelines and acceptable staff. Each organization will want to adapt
industry best practices to its unique markets and context, as ideal hiring and retention plans
address the unique needs of the organization (e.g., focusing on being able to hire from new
locations or new candidate profiles, focusing on increasing the number of applicants by
raising awareness).
This section describes:
1. Levers to support recruitment
2. Levers to support retention
1. Levers to support recruitment
This section includes resources and information about:
• Job boards and postings
• Compensation
• Job requirem
ents
• Expanding geographic areas for recruitment
• Working models
• Operations
• Identifying partnership opportunities t
o identify new sources of talent
Expanding use
of job boards / websites: Assess how and where jobs are posted and
advertised:
• Identify the standard list of places the positions are posted; li
sts of job boards /
websites can be found on the web including thi
s resource from Better Team
(https://www.betterteam.com/free-job-posting-sites)
10
• Ask employees where they heard about the organization and make sure the
opportunities are posted there
• Reach out
to partner health care organizations to identify potential new channels to
advertise positions
• Identify ways to make the position stand out: Wh
y should people choose this
organization? What makes working at this organization different?
9
National Suicide Prevention Lifeline, “Call center metrics,” pgs. 54-64, accessed February 7, 2022.
10
“21 free job posting sites that are high traffic and 100% free,” Betterteam. accessed February 24, 2022,
https://www.betterteam.com/free-job-posting-sites.
22

• Consider adding a resume bank to a career’s page to allow utilization of an applicant
management system feature to match applicants from previous positions or resume
bank to open employment opportunities, as appropriate
Case study: Behavioral Health Response (BHR)
(Missouri)
11
BHR uses a variety of tools to recruit top candidates, including:
• Indeed
: htt
ps://www.indeed.com/ - Indeed is a very broad recruiting website that a
vast majority of job seekers use to find positions—regar
dless of the industry
• Zipr
ecruiter: ht
tps://www.ziprecruiter.com/ - ZipRecruiter is another very broad
recruiting website that a lot of job seekers use
• Li
nk
edIn Careers: htt
ps://careers.linkedin.com/ - LinkedIn Careers is a tool used to
hire more professional-level
roles (i.e., management or hyper-specialized
professional roles). Many
clinicians in non-management roles have also used
LinkedIn to find employment
• The R
om
e Group: https://www.theromegroup.com/ - The
Rome Group is a
recruiting tool for non-prof
it jobs but is area specific
• Ac
ademic institutions as well as professional networking organizations such as
area c
hambers can provide sources of local talent
•
C
hambers: Chambers of Commerce, including those representing individuals from
diverse backgrounds, can serve as potential sources of talent
Case study: Lines for Life (LFL) (Oregon)
12
LFL considers many job boards / websites for job posting, including Indeed Career
Builder, Handshake, ZipRecruiter, and LinkedIn. To succ
essfully source a candidate on a
platform, it is important to identify the candidate’s prio
rities.
• Boolean search: if a center wants to hire a Crisis Call taker, it might type “crisis
AN
D call taker” into the search bar and include the location. This is called a
Boolean search term and it filters
th
rough candidates to reach out to them directly.
Another example is “MH AND
nonprofit.” Indeed allows a search to be narrowed
down to include only people that have recently updated their profiles, level of
experience, level of education, and any assessments t
aken
• Templ
ates: Most sourcing platforms will have an option to save a template, so job
desc
riptions do not have
to be recreated. The most important elements should be
at the top of the template (e.g
., job title, status (full time / part time / temporary /
permanent), location, and compensation)
•
T
itle: When posting a job, it is important to include the title of the job throughout
the pos
ting. For example: Crisis Call Taker Position Summary, Crisis Call Taker
Responsibilities, Crisis Call Taker Requirements, Crisis Call Taker Physical
Requirements, and so on. This is so the title and key words are more frequent and
match the algorithms so that the job is more likely to be found by someone
seeking it out. If a job posting is not getting enough applicants, consider whether
the title would be attractive to job seekers
11
Bart Andrews, Vice President of Clinical Practice / Evaluation at Behavioral Health Response, February 2022.
12
Dwight Holton, CEO of Lines for Life, February 2022.
23

• Personalization: LFL found that candidates are more likely to be interested in
outreach if a name is included in the email. Candidates can tell the difference
between generic and personalized outreach and are less likely to look at generic
outreach
• Review for bias: Review the post to ensure there are no gendered phrases or
biased speech in the post, e.g., “workmanship” and “manpower”
Case study: Solari (Arizona)
13
Like most contact centers, Solari is also feeling the effects of the recent applicant
shortage and the reverberation of what is being referred to as the “Great Resignation.” In
response t
o the COVID-19 pandemic in 2020,
Solari remotely hired and trained more than
250 staff in four months to meet the needs of the community through center service
s.
Solari applies a continuous recruitment strategy to center positi
ons. Its talent acquisition
team is open to receiving and reviewing applications regardless of position vacancy. This
creates a bench of qualified applicants and allows the team to stay in touch with local job
m
arkets, positively impacting time-to-fill m
etrics. Positions are posted on the Solari
website, which are captured by Indeed,
Glassdoor, and Diversity.com web scrapers.
These sites serve as placeholders and information passthroughs, increasing visibility a
nd
reach. The agency als
o collaborates regularly with local universities on projects to
maintain its expert
ise in the crisis space.
Solari’s headquarters are in the fifth largest city in the country, which provides a robust
pipeline of candidates. Its recr
uitment process is streamlined and includes an initial
review by a seasoned member of the center team. Thi
s assistance with resume review
and initial phone interviews helps identify appropriate candidates for the role.
Compensation
: Compensation can generally be aligned with mean / median wages and
adjusted for location, when possible. Before beginning any compensation assessment,
Centers would start with a clear organizational chart with accurate job descriptions for each
position and determine how broad the benchmark should be.
Centers could utilize a cost per contact of $82 to calibrate their center-level costs, according
to the SAMHSA 988 appropriations report
(https://www.samhsa.gov/sites/default/files/988-
appropriations-report.pdf
)
14
This estimate of cost per contact accounts for:
• “Dedicated resources (i.e., crisis workers and their supervisors)
• Shared resources (i.e., center direct
or, HR manager) that support other programs in
addition to 988
• Dedicated capital (assets employed for the sole use of 988)
• Shared capital (assets used by multiple programs administered by the network
center)
• Dedicated expenses (expenses incurred to support 988, AAS conference)
• Shared expenses (expenses incurred to support the network center, e.g., rent)
13
Justin Chase, President and CEO of Solari Crisis and Human Services, January 2022.
14
Substance Abuse and Mental Health Services Administration, “988 appropriations report,” December 2021: pg. 10,
https://www.samhsa.gov/sites/default/files/988-appropriations-report.pdf.
24

• Common center processes are also calculated in the model (refresher training,
quality, debrief sessions, and attrition)”
15
To conduct a
compensation evaluation, centers can:
• Determine a benchmark f
or direct salary costs for crisis counselors by reviewing
potential benchmarks and considering a market study. Potential benchmarks may
include:
o The B
ureau of Labor Statistics (BLS), which breaks down wages (hourly and
annual; percentile) by geography (state, metropolitan area) and includes
related roles:
BLS roles
Psychiatric Technicians
16
Psychiatric Aides
17
Social and Human Service Assistants
18
Substance Abuse, Behavioral Disorder, and MH Counselors
19
and Substance Abuse Social Workers
20
Customer Service Representatives
21
o Government entities such as state-level classification schedules
• Assess benefits packages for competitiveness (e.g., retention bonuses, paid time off,
r
emote working options, childcare programs) and adjust as needed. Consider
improving benefits packages as tenure increases
• Assess financial incentives such as offering hiring bonuses, referral bonuses, and/or
tuition reimbursement
Case study: Integral Care (Austin, Texas)
22
Integral Care recently standardized its compensation practices. Historically,
compensation practices were somewhat but not fully standardized for all posts with a
common benchmark. Integral Care’s leadership and human resources decided to try to
use one external benchmark and s
elect
ed the Texas State Auditors’ classification
schedule because it is external, validated by government, and updated regularly (~every
two years).
15
Ibid.
16
“Occupational employment and wages: May 2020 29-2053 Psychiatric Technicians,” Bureau of Labor Statistics, modified
March 31, 2021, accessed February 7, 2022, https://www.bls.gov/oes/current/oes292053.htm.
17
“Occupational employment and wages: May 2020 31-1133 Psychiatric Aides,” Bureau of Labor Statistics, modified March 31,
2021, accessed February 7, 2022, https://www.bls.gov/oes/current/oes311133.htm.
18
“Occupational employment and wages: May 2020 21-1093 Social and Human Service Assistants,” Bureau of Labor Statistics,
modified March 31, 2021, accessed February 7, 2022, https://www.bls.gov/oes/current/oes211093.htm
19
“Occupational employment and wages: May 2020 21-1018 Substance Abuse, Behavioral Disorder, and Mental Health
Counselors,” Bureau of Labor Statistics, modified March 31, 2021, accessed February 7, 2022,
https://www.bls.gov/oes/current/oes211018.htm.
20
“Occupational employment and wages: May 2020 21-1023 Mental Health and Substance Abuse Social Workers,” Bureau of
Labor Statistics, modified March 31, 2021, accessed February 7, 2022, https://www.bls.gov/oes/current/oes211023.htm.
21
“Occupational employment and wages: May 2020 43-4051 Customer Service Representatives,” Bureau of Labor Statistics,
modified March 31, 2021, accessed February 7, 2022, https://www.bls.gov/oes/current/oes434051.htm.
22
Rodney Guinn, Director, Human Resources at Integral Care, February 2022.
25

Each role was evaluated and matched to the benchmark by multiple factors, including
level, education, supervision, budget responsibilities, initiative, and risk. Integral Care
determined that each job could be placed
on a midpoint within the benchmark range, and
that point varied based
on the role and/or an individual’s experience. Additionally, Integral
Care contracted a vendor
to evaluate market conditions, given the increasing cost of
living in its location (Austin) and shifting co
mpensation demands from potential
candidates.
Job requi
rements and working models: Centers can evaluate how different job
requirements and working model expectations are impacting hiring and consider adjustments
as appropriate, including:
• Assess current j
ob description requirements and compare them to similar roles.
Determine if any requirements can be adjusted to broaden the potential applicant
pool including:
o Entry level: C
onsider minimum requirements for entry-level jobs to allow
substitutions for formal education and/or mandatory training to enable hiring
from alternative pathways
o Licensing: The Li
feline does not require specific licensing of crisis counseling
team members at centers and team members may be volunteers, depending
on other requirements (e.g., local, state, other funders)
o Experience: C
onsider expanding historical education and experience
requirements to include a broader group of potential applications (e.g., first
responders, police, emergency management services, 911 responders)
o Other requirements: R
eassess job requirements that may be overly
restrictive, based on best practices and state guidance
• Identify ways to expand the geographic area from which the center can hire (e.g.,
hiring across state and country, when possible). During COVID-19, many centers
transitioned to virtual service provision and looked to hire beyond the county or state
• Explore non-t
raditional work models including remote, hybrid, and/or split models (two
employees working partial hours that coordinate schedules to fulfill hours requirement
of one FTE) that may be more broadly appealing. Also consider utilizing overtime /
comp-time in calculating overall FTE organizational needs
New sources of talent: Centers could also expand the pool of talent from which they draw
applicants by:
• Identifying cr
eative pathways in communities, for instance by partnering with local
universities and community colleges to raise awareness and by offering internships
and work study programs
• Expandi
ng recruiting of and the roles of people with lived experience in the
center across levels. Reach out to organizations that train and identify people with
lived experience at the local level as well as national organizations that offer peer
support training programs and have trained thousands of peers (e.g., RI International
and Mental Health America).
23
The National Association of Peer Supporters (NAPS)
also has a job board
(https://www.peersupportworks.org/) that c
an be used to share
jobs with peers. Additional resources for organization’s hiring Peer Workers can be
23
“MHA announces partnership on peer support with RI International,” Mental Health America. accessed February. 7, 2022,
https://mhanational.org/blog/mha-announces-partnership-peer-support-ri-international.
26

found on SAMHSA’s Peers page (https://www.samhsa.gov/brss-tacs/recovery-
support-tools/peers)
24
Hiring oper
ations: Centers can also assess the speed to hire of recent hires and identify
potential points in the process where they can shorten the recruitment timeline. If there is a
part of the process (e.g., round of interviews with senior staff) that regularly takes longer than
planned, evaluate whether that process can be accelerated or potentially replaced.
2. Levers to support retention
This section includes resources and information about:
• Career development
• Supervision / licensure hours
• Workforce protection and staff well-being
Career development: Building a culture of investment in team members’ career
development can help support retention. This can involve:
• Holding senior team members accountable for prioritizing mentorship
• Building connections between team members and supervisors
• Building cohort or discipline-based acti
vities or workshops to foster a sense of
community among team members. For example, have all new hires start on the same
day to build community and have a member of that group coordinate regular (e.g.,
monthly or quarterly) trainings, speaker sessions, and/or social events
Supervision
/ licensure hours: Offering supervision / licensure hours to team members, as
allowed by the state, can help to retain employees who are simultaneously seeking licensure.
Some states, including Georgia, allow crisis contact hours to count for licensure.
Workforce protection and staff well-being:
25
Center staff that answer the Lifeline are
routinely exposed to traumatic material such as severe human distress and highly disturbing,
graphic material including abuse, despair, hopelessness, and violent death. This continuous
exposure has the potential to cause negative psychological effects such as compassion
fatigue / secondary traumatic stress, sleep problems, a change in their view of the world as a
good and safe place, and, less commonly, even mental illnesses such as depression and
posttraumatic stress disorder (PTSD).
26
These stress
ors can impact staff’s decisions as to whether and how long they remain
working in a particular center and also in the field in general. There is early research
indicating centers experience a high turnover of volunteers and staff when the call volume
increases in relation to suicide calls. Employees who are in good physical, mental, and
emotional health are more likely to deliver optimal performance in the workplace than
employees who are not, and ultimately healthy, well-prepared, and well-trained staff reduce
turnover rates.
27
The ripple effects of reduced turnover rates are the positive effect of less
24
“Peers,” Substance Abuse and Mental Health Services Administration, accessed February 7, 2022,
https://www.samhsa.gov/brss-tacs/recovery-support-tools/peers.
25
April Naturale, Assistant Vice President, National Programs, and Assistant Vice President, National Crisis & Wellness
Programs at Vibrant Emotional Health, February 2022.
26
C.R. Figley, (1999). “Compassion fatigue: Toward a new understanding of the costs of caring,” in Secondary traumatic stress:
Self-care issues for clinicians, researchers & educators, ed. B. H. Stamm, (Baltimore: Sidran Press, Second edition 1999), 3-
29; Laurie Anne Pearlman and Paula A. Mac Ian, “Vicarious traumatization: An empirical study of the effects of trauma work
on trauma therapists,” Professional Psychology: Research and Practice, 26, no. 6, (1995): 558-565,
https://www.nationalcac.org/wp-content/uploads/2016/10/Vicarious-traumatization-An-empirical-study-of-the-effects-of-trauma-
work-on-trauma-therapists..pdf.
27
Jerome M. Adams, “The value of worker wellbeing,” Public Health Reports 134, no. 6 (November 2019): 583-586,
https://doi.org/10.1177/0033354919878434.
27

strain on the staff, faster response rates, and the ability to keep these valuable resources
answering lifesaving calls in the local community.
28
Centers can
take steps to improve staff wellbeing and engagement, including:
29
Areas Capabilities
Measure and track
org
anization health and
employee satisfaction
• Assess availability and adequacy of current employee wellbeing
program offerings, and add capacity or new resources as needed
• Weekly pulse surveys for center staff to voice concerns and suggest
potential change to ways of working
• Annual / bi-annual employee engagement survey to measure
perceptions and experiences of center counselors (e.g., work
environment, motivation, culture, likelihood to stay)
• Annual / bi-annual organizational health survey to gain insights into
organizational culture, management practice, and the effectiveness of
operational processes
In
troduce programs an
d/or
benefits to promote staff
well-being
• On-site wellness counselors and quiet meditation rooms to
promote staff resiliency
• Greater staff flexibility through shorter shift times, frequent breaks,
more paid vacation days, and alternative work schedules (e.g., part-
time, staggered shift hours)
• Expand behavioral health (BH) benefits for all network staff
through employee assistance programs (EAP) and/or by partnering
with existing wellness apps
• Staff engagement programs (e.g., peer networks, buddy
assignments) to build a culture of collaboration and teamwork
• Stress management trainings and coaching sessions to share
best practices, tips, and tricks among staff members (e.g., staying in
balance workshop series for healthy solutions to workplace stress)
Bu
ild engagement and
awaren
ess around
wellness programs
• Regular and clear communications with center staff through
emails, newsletters, and local events on available resources and
when / how to access them
• Ensure clear communications on the importance of employee
wellbeing at all levels and normalize team conversations regarding
situational distress
• Quick and transparent process for sharing results from employee
engagement and organization health surveys with all network staff
• Network-wide workshops and facilitated team discussions to
check-in, surface distress, and share ideas to improve counselor
wellbeing
• Collection of insights and learnings from other companies that are
experienced in implementing successful employee wellbeing
programs
Resources f
or frontline workers and their families that will support the center workforce’s
resiliency can be found in the National Alliance on Mental Illness’s (NAMI’s) Frontline
Wellness Initiative (http
s://www.nami.org/Your-Journey/Frontline-Professionals).
30
28
Derek Rouch and Liz Barnes, “Crisis at CrisisLink: Increasing the retention rate for crisis workers answering a suicide crisis
line,” Leadership and Learning in Organizations Capstone Projects, Vanderbilt University Institutional Repository, April 4,
2021, http://hdl.handle.net/1803/16527.
29
Interview with Vibrant, 2022
30
“Frontline professionals,” National Alliance on Mental Illness, accessed February 7, 2022, https://www.nami.org/Your-
Journey/Frontline-Professionals.
28

Case study: Behavioral Health Response
(BHR) (Missouri)
31
BHR utilizes best practice models for workforce retention that include the following:
• Exit interviews: Conducts exit interviews with staff who are leaving the
organization. This is a useful tool to understand what is going right and what is
going wrong. Additionally, it helps to identify reasons why staff are leaving and
helps to identify themes that organizations need to address. This information can
be shared with decision-makers to make effective changes within the organization
• Stay surveys: Surveys
the current workforce to identify issues that can be
addressed quickly to retain existing staff and to determine which ongoing
initiatives are most effective
• Communications: Ho
lds regular, productive team meetings at all levels to ensure
that everyone is on the same page. All-staff meetings allow colleagues to
participate in discussions on the organization’s direction and how they can be a
part of that mission, vision, and strategy, which can be helpful in gaining and
strengthening buy-in
• Team engagement: Engages s
taff throughout the year by celebrating holidays,
having luncheons, and setting up meetings. These events allow team members to
engage with each other in non-stressed, social settings
• Employee c
ommittees: Forms committees of employees across departments to
offer real-time feedback on what can be done to better engage and retain team
members
• Compensation analysis: C
onducts a third-party compensation analysis to ensure
posi
tions are being compensated appropriately for the market, if compensation is
a reason staff are leaving and the organization has a large enough budget
Case study: Lines for Life (LFL) (Oregon)
32
LFL is working on employee retention, beginning with employee recruitment, hiring, and
onboarding. Practices that have worked for LFL include:
• Hiring process: Using a hiring process that ensures employees understand the
nature of the work
• Interventions and surveys: Utilizing e
xit
interviews, stay interviews, and employee
surveys to find out what is important to employees as a group and individually
o This
information helps LFL unders
tand why people leave organizations.
Management often thinks it
is for pay, but this is only part of the picture and
not the primary reason employees report for leav
ing
•
Culture: Understanding the importance of culture and setting the tone for a
positive, mission-driven culture from the top
31
Bart Andrews, Vice President of Clinical Practice / Evaluation at Behavioral Health Response, February 2022.
32
Dwight Holton, CEO of Lines for Life, February 2022.
29

•
Benefit surveys: Doing regular benefit surveys to ensure that the organization
stacks up well. This is crucial because today’s job market is an employee’s
m
arket. LFL has found most comparable employers offer health, dental, vision,
short- and
long-term disability and life insurance. Paying for these in full or near
full is the expectation of, not
the exception for, many potential applicants
•
Professional development: Developing a structured program for employees to
l
earn and grow in their positions and in the organization. Employees have
expressed interest in development and career growth
•
Leader
ship training: Providing training for supervisors in how to coach and lead
em
ployees. Frequently people are advanced to
higher roles in organizations
because they are good
at what they currently do, which does not automatically
translate into being good at supervision
•
Flexibility and autonomy: Developing opportunities to provide flexibility, such as
part-time employment, four ten-hour shifts (“4/10’s”), or other non-traditional
schedules. Employees want flexibility and autonomy. This can be challenging with
shift work
Case study: Solari (Arizona)
33
Solari has a very active Social Employee Engagement Committee (SEEC) that is
dedicated to engaging, encouraging, and exciting staff along their journey. It recognizes
that when staff feel cared for and appreciated, their fulfillment will fuel the services they
provide to crisis line callers, and they will more likely remain in their positions. SEEC
regularly plans in-person and virtual events to keep staff connected and allow space to
decompress and laugh with each other. Such sponsored events and activities include
spirit weeks, book clubs, bingo nights, costume challenges, wellness challenges,
quarterly lunches, self-care challenges, guided meditations, fitness subscriptions,
massage days, and more. Solari recognizes that self-care is individualized, and the
organization aims to provide ample opportunities for employees to focus on their
wellbeing.
In addition, Solari provides a comprehensive benefit package that includes a 401(k) with
employer match, 13 annual paid holidays (which include two Solari Wellness days), paid-
time off accrual with annual payout and rollover policies, public student loan forgiveness,
tuition reimbursement, an on-site fitness room, and on-site fresh vending. It recognized
early in the pandemic that staff members required additional self-care strategies and
flexibility due to the stressful nature of their jobs and the increased stress and uncertainty
of being in a global pandemic. Solari immediately implemented an updated staffing model
that included work from home and more flexible schedules. It also offered an enhanced
fiscal reward coupled with additional time off to provide much needed recognition and
reprieve.
Finally, Solari’s Chief Administrative Officer is an active participant on The Lifeline Cares
Advisory Committee and works in partnership with the human resources team to
continually advance Solari’s investment in i
t
s people. The agency uses a 30-60-90-day
check in process for new employees and has created a
transparent exit interview system
to ensure it is
capturing the reasons staff are leaving the organization. It provides this
information to both line-level leadership and the executive team to ensure full visibility.
33
Justin Chase, Solari, February 2022.
30

Solari is also pursuing a continuous quality-improvement (CQI) approach to engage,
support, and motivate center staff to support themselves and each other.
Additiona
l resources
• Vibrant’s
Crisis Center Metrics
(https://suicidepreventionlifeline.org/wp-
content/uploads/2019/02/CallCenterMetrics_final.pdf)
34
• North American Quitline Consortium’s (NAQC’s) Fundamental
s of Call Center Staffing
and Technology
(https://cdn.ymaws.com/www.naquitline.org/resource/resmgr/issue_papers/callcenter
metricspaperstaffi.pdf)
35
• Communities of practice (for best practices)
o National Association of Crisis Organization Directors
(https://www.nascod.org/about)
o International Council for Helplines
(https
://councilforhelplines.org/)
o American Association of Suicidology
(suicidology.org)
34
National Suicide Prevention Lifeline, “Crisis call center metrics,” accessed February 7, 2022.
35
Penny Reynolds, (2010). “Fundamentals of call center staffing and technologies: Quality improvement initiative,” North
American Quitline Consortium, 2010,
https://cdn.ymaws.com/www.naquitline.org/resource/resmgr/issue_papers/callcentermetricspaperstaffi.pdf.
31

2. Financial sustainability
I
n 2022, SAMHSA began providing funding to centers through the 988 State and Territory
Grant program to provide workforce-related support. “The purpose of these cooperative
agreements is to improve state and territory response to 988 contacts (including calls, chats,
and texts) originating in the state / territory by:
1. Rec
ruiting, hiring, and training BH workforce to staff local 988 / Lifeline
centers to respond, intervene, and provide follow-up to individuals experiencing a BH
crisis
2. Engagi
ng Lifeline crisis centers to unify 988 responses across states / territories
3. Ex
panding the crisis center staffing and response structure needed for the successful
implementation of 988
It
is expected that these grants will:
1. Ens
ure all calls originating in a state / territory first route to a local, regional, and/or
statewide Lifeline crisis call center
2. Im
prove state / territory response rates to meet minimum key performance indicators
3. Inc
rease state / territory capacity to meet 988 crisis contact demand”
36
To hel
p ensure that the Lifeline crisis centers are able to recruit and respond to the 988
demand, no less than 85 percent of grant funds must be allocated to selected local, regional,
and/or statewide Lifeline crisis centers and used for workforce capacity and related
expenditures.
37
As
the Brookings Institute’s “Building a Sustainable Behavioral Health Crisis Continuum”
states: “ensuring adequate financing both for the initial call response and connecting people
who need them to services will be a key determinant of the availability and effectiveness of
crisis response services.”
38
Federal law allows states to finance call center operations
through a fee on cell carriers; however, only a handful of states have enacted legislation to
date.
39
As of March 2022, enacted or proposed 988 legislation is tracked in this dashboard
(https://www.quorum.us/dashboard/external/mgWzdPqJLWHohzOhdRWE/).
To ensure f
inancial sustainability over time and the ability to meet the needs of individuals in
crisis, it will be key for Lifeline contact centers to access diverse and long-term funding
streams.
This section addresses opportunities for Lifeline contact centers to
• Identify additional sources of funding
• Improve insurance billing capabilities
36
Department of Health and Human Services and Substance Abuse and Mental Health Services Administration, “FY 2022
cooperative agreements for states and territories to build local 988 capacity,” accessed February 2022,
https://www.samhsa.gov/sites/default/files/grants/pdf/sm-22-015.pdf.
37
Ibid.
38
Richard G. Frank and Vikki Wachino, “Building a sustainable behavioral health crisis continuum,” USC-Brookings Schaeffer
on Health Policy, January 6, 2022, https://www.brookings.edu/blog/usc-brookings-schaeffer-on-health-
policy/2022/01/06/building-a-sustainable-behavioral-health-crisis-continuum/.
39
“Text – S.2661 – 116
th
Congress (2019-2020),” October 17, 2020.
32
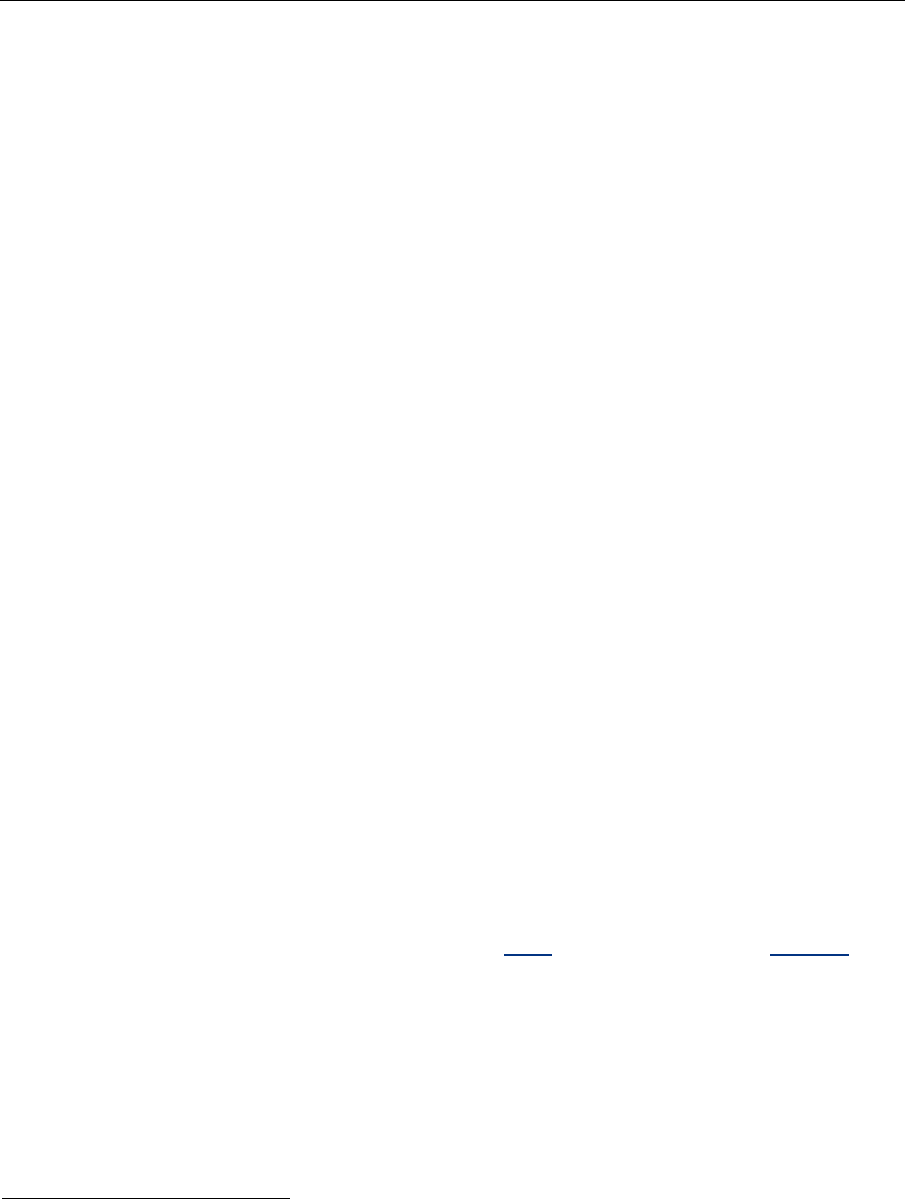
Resources to identify potential sources of ongoing funding
and build diverse funding sources
H
HS resources that support 988 and crisis services include:
40
S
AMHSA
• 988 State and Territory Cooperative Agreement (12/2022)
• Community Mental Health Services Block Grant —
5 percent Crisis Services set-
aside
• Certified Community Behavioral Health Center (CCBHC) grant
• Zero Suicide Grant
• Garrett Lee Smith Youth Suicide Prevention (GLS) Grant
• Rural Emergency Medical Services Grant
• State Opioid Response (SOR) Grant & Tribal Opioid Response (TOR) Grant
• Tribal Behavioral Health Grant (Native Connections)
• State Transformational Technology Initiative Grants
(Tr
ansformation Transfer Initiative – National Association of State Mental Health
Program Directors (TI-NASMHPD))
• Governors’
Challenges to Prevent Suicide Among Service Members, Veterans, and
their Families
SAMHSA Technical Assistance
• Suicide Prevention Resource Center
• Center of Excellence for Integrated Health Solutions
• National and Regional Mental Health Technology Transfer centers
• GAINS Center for Behavioral Health and Justice Transformation
• Nati
onal Child Traumatic Stress Network
CMS
• Medicaid / Chi
ld’s Health Insurance Program (CHlP) Waivers - 1915 and 1115
• Medicaid / C
HlP State Plan Amendments
• CMS State Planning Grants for Qualifying Community-B
ased Mobile Crisis
Intervention Services ($15M for 20 states)
In addi
tion to information from SAMHSA, the NSPL NRC includes a section on Funding
resources
(https://networkresourcecenter.org/plugins/servlet/samlsso?redirectTo=%2Fpages%2Fviewp
age.action%3FspaceKey%3Dpracticeguide%26title%3DTip%2BSheets).
41
The NRC outlines
current and previous funding opportunities, and describes a mix of funding sources that can
be considered, including fees for service structure, funding opportunities to join specific sub-
networks, and new Lifeline grants.
40
Input from SAMHSA, 2022.
41
Network Resource Center, National Suicide Prevention Lifeline, accessed Feb. 25, 2022,
https://networkresourcecenter.org/plugins/servlet/samlsso?redirectTo=%2Fpages%2Fviewpage.action%3FspaceKey%3Dincallt
ools%26title%3DIn-Call%2BTools.
33

Improving insurance billing capabilities and related
considerations
I
nsurance billing capabilities
Setting up and expanding insurance capabilities is an investment of time and resources, but
can be worthwhile, particularly in states with a federal match. Variation exists among states
in the extent to which Medicaid is currently used to cover crisis services, including crisis
hotline calls and mobile crisis services.
Providers could utilize Medicaid reimbursement from a state, if available.
42
It will be
necessary to coordinate with the State Medicaid authority to identify the current status of
Medicaid reimbursement for crisis contact services, which varies by state.
43
If unclear, it is
possible to ask the Medicaid authority if / what billing code(s) are active in the state, including
the BH hotline services (H0030).
44
Example: Arizona
45
In September 2001, the Arizona Department of Health Services Division of Behavioral
Health Services released their Covered Behavioral Health Services Guide. It included
specific billing procedures for Telephonic Crisis Intervention Services and used the Case
Management Healthcare Common Procedure Coding System (HCPCS) procedure code
T1016. Contact centers collaborated with the State of Arizona and local entities on setting
up the program.
As a result of the program, 58 percent of crisis call volume was Medicaid-reimbursed in
2021.
R
eimbursement and billing considerations
46
The I
nsurance Reimbursement Guidance
(https://networkresourcecenter.org/plugins/servlet/samlsso?redirectTo=%2Fpages%2Fviewp
age.action%3FspaceKey%3Dpracticeguide%26title%3DTip%2BSheets
) in the NRC outlines sever
al considerations related to reimbursement, including the
importance of:
• Ensuring consent and transparency
• Following clear policies / procedures to explain information sharing
• Focusing on the cr
isis intervention and the safety assessment model
Sp
ecifically, “Centers must be careful about assuming that callers / chatters / texters will
endorse the understanding that the service is ‘free’ if only their insurance is charged. Centers
42
“Guide to Medicaid billing,” Crisis Response Network, 2021.
43
The Federal government allows states to offer Medicaid reimbursement for certain community-based behavioral health
services like crisis contact services, but not all states offer crisis call reimbursement. This is generally done through 1115
Medicaid Demonstration Waivers.
44
The behavioral health hotline is a telephone service that provides crisis intervention and emergency management such as
mental health referrals, treatment information, and other verbal assistance.
45
Interview with RI International, January 2022.
46
“Vibrant and 988,” Vibrant Emotional Health, July 13, 2020, accessed March 8, 2022, https://www.vibrant.org/988/.
34

must offer a clear understanding of their center policies and practices to contacts so that they
may make an informed choice about using the service.”
47
Consent
and transparency: According to Vibrant, billing practices must include consent and
transparency. Individuals have a right to know when and how their information is going to be
shared. Centers may not collect information without clearly explaining what it will be used for
and gaining explicit consent.
48
Pol
icies and procedures: If a center will be seeking insurance reimbursement for crisis
conversations, there must be a policy / procedure in place to clearly explain to the individual
what information will be shared, who it will be shared with, and how it will be used. The
center should explain that the individual has the right to refuse consent, and they will still
receive the same services from Lifeline / 988. For example, consent to share / bill must be
opt-in and indicated in the documentation for each individual conversation that is billed.
49
Focus: Cr
isis intervention and the safety assessment model must remain the primary focus.
Centers cannot screen out individuals based on their decision to consent / not consent to
insurance reimbursement. Any identifying information that will be used for billing /
reimbursement purposes should not be collected at the beginning of the crisis conversation
prior to establishing rapport. Centers cannot refuse services or end conversations
prematurely if an interaction is reaching the time or service limit of what can be billed /
reimbursed.
50
Addit
ional information: Consult the Gathering Demographics While Maintaining Rapport tip
sheet on the NRC
(https://networkresourcecenter.org/plugins/servlet/samlsso?redirectTo=%2Fdashboard.action).
47
Vibrant Emotional Health, “ 988 serviceable populations and content volume projections,” December 20, 2021, accessed
February 7, 2022, https://www.vibrant.org/wp-content/uploads/2020/12/Vibrant-988-Projections-
Report.pdf?_ga=2.62739180.1718066263.1611784352-1951259024.1604696443.
48
“988 insurance reimbursement guidance from the Network Resource Center,” Vibrant Emotional Health, 2021 accessed
February 7, 2022.
49
“988 insurance reimbursement guidance from the Network Resource Center,” Vibrant Emotional Health, 2021 accessed
February 7, 2022.
50
“988 insurance reimbursement guidance from the Network Resource Center,” Vibrant Emotional Health, 2021 accessed
February 7, 2022.
35

3. Connection to 911 / PSAPs
Strong r
elationships between PSAPs—call centers responsible for answering calls to 911—
and Lifeline contact centers are essential to realize the full potential of 988 and better serve
individuals in crisis. 988 and 911 are designed to be complementary. As articulated by the
National Emergency Number Association (NENA), “988 counselors are trained to utilize the
least invasive interventions whenever possible, and ongoing collaboration between 988 and
911 will help individuals in crisis get the appropriate support, providing options like MCTs in
place of police or EMS responders when needed and where available.”
51
The ultim
ate goal of collaborative relationships between crisis centers and PSAPs is
increased safety for those at imminent risk of suicide in the community.”
52
This includes:
•
“Better and more compassionate care for individuals at risk of suicide that utilizes
best and recommended practices
• Improved workflows that decrease staff frustration and burnout
• Community support through the partnership and 911’s championing of the crisis
center services is crucial, as well as the PSAPs’ ability to provide timely and safe
responses to all callers”
53
Mater
ial tailored specifically to PSAPs is available in the PSAPs 988 Convening Playbook.
Process to develop relationships with PSAPs
Relati
onships between Lifeline contact centers and PSAPs often begin with informal
engagement and processes and then evolve to formal relationships created via
Memorandums of Understanding (MOUs) or Business Associate Agreements (BAAs). Steps
for engaging PSAPs include:
• Identify and reach out to your local PSAPs in the community, use the Lifelines NRC.
54
Begin with PSAPs that are geographically closest and then expand to PSAPs that
are
located farther away
(https://networkresourcecenter.org/plugins/servlet/samlsso?redirectTo=%2Fdashboar
d.action)
• Focus
on building and/or improving processes related to: (a) transferring calls from
the
PSAP to the contact center, and (b) transferring calls from the contact center to
the PSAP. The NENA
Suicide/Crisis Line Interoperability Standard may be a helpful
starting off point for relationship building
(https://cdn.ymaws.com/www.nena.org/resource/resmgr/standards/nena-
sta
-001.2-2022_suicide-.pdf)
• Codify pr
ocesses in a formal arrangement such as a MOU
or BAA. Two sample
MOUs are included in the Appendix,
one a simple template and another specific for
centers
that are blended crisis / information and referral lines
Inform
al understandings or formal agreements can contain approaches to address:
51
National Action Alliance for Suicide Prevention, “988 messaging framework–Draft” (unpublished manuscript, January 21,
2022).
52
Caitlyn Peterson and Shye Louis, “Addressing imminent risk via collaborative 911 relationships and the NENA Suicide
Prevention Standard” (PowerPoint presentation, National Crisis Center Conference, St. Louis, MO, October 18, 2018),
https://www.crisiscon.org.
53
Caitlyn Peterson, “Addressing imminent risk,” October 18, 2018.
54
“PSAP (911) locator,” Vibrant Emotional Health, n.d., https://networkresourcecenter.org/display/incalltools/In-Call+Tools.
36

• Specific processes to transfer calls from a PSAP to a contact center
• Specific process to transfer calls from a center to a PSAP, including potentially a
direct line between the crisis call center and the PSAP so those calls are labeled as
crisis calls
• Data sharing approach (e.g., what data is shared)
• Systems and interoperability
Transfer of calls from 911 to 988
Protoc
ols for transfer of calls from 911 to 988 are unique to specific PSAPs and Lifeline
contact centers. In general, protocols will need to address multiple topics, including but not
limited to:
• Situations that can be considered for transfer
• Times of day that calls can be transferred (if relevant)
• Approach to warm transfer and example script for PSAP operators
• Approach to transferring caller data
• How Lifeline contact center operators should handle the call
An example
“911 dispatch protocol for diverting calls involving persons experiencing a MH
crisis to a crisis center” from Didi Hirsch can be found in the Appendix
.
Centers
can share additional information about setting up and/or improving existing
protocols.
Transfer of calls from 988 to 911
Lifeli
ne centers will not generally transfer 988 callers who are currently in progress of suicide
or at imminent risk to 911 to handle directly. Rather, a supervisor or colleague at the center
will contact the PSAP for assistance on behalf of the person needing intervention while the
crisis counselor continues to interact with the person needing intervention as long as they
can be kept on the line (until intervention arrives).
55
As laid out in the NENA 911-988
workgroup’s 988 to 911 Transfer draft, transfers from 988 to 911 may occur in the following
cases:
• Ability to share location information: “If the person needing intervention is willing
and able to provide clarification on their location to receive help. (The 988-crisis
counselor may stay on the line in these cases, but will inform the 911
telecommunicator if they intend not to disconnect after transfer)
• Third-party callers: A third-party caller is someone who is seeking help for someone
else. If a third party is reporting imminent risk / attempt in progress of someone they
know, 988 may warm transfer the third-party caller to 911 so they can give more
direct information about the person needing intervention to the PSAP. (The 988-crisis
counselor would opt for transfer when it is unclear whether the third-party caller will
follow through with calling 911 themselves to provide this information)
• Emergencies not related to suicide: Sometimes in the course of a 988 interaction
about mental health or emotional distress, another emergency situation may be
55
Shye Louis, Director of Clinical Best Practices at Vibrant Emotional Health, February 2022.
37

disclosed outside of suicide but that requires life-saving intervention, such as a
medical emergency or a violent crime in progress / imminent:
o When assessed as safe to do so, a 988 center can direct those callers to hang
up and dial 911 f
or assistance, so the 911 center can get correct location
information
o There may be times where it does not seem safe to have the
person call 911;
the 988-crisis counselor may then warm transfer the person to 911 to ensure
that they contact emergency assistance.”
56
For more inf
ormation on this process please refer to the Suicide / Crisis Line Interoperability
Standard (currently in Stable Form Notice 30-day period).
57
An example “LAPD 911
diversion guide for SPC counselors and supervisors" from Didi
Hirsch can be found in the Appendix
.
Data-sharing approach
As stated
in the NENA Suicide / Crisis Line Interoperability Standard: “Sharing of data
between 911 and other entities within the crisis ecosystem can be critical for enabling the
right response at the right time for individuals in crisis. Both critical incident data and caller
information (e.g., caller ID, address, IP address) would ideally be able to be shared with
partners, including Lifeline contact centers and first responder agencies.
Regulations currently do not limit data
sharing between PSAPs and 988. PSAPs are legally
permitted to obtain or request that a mobile carrier obt
ain the geolocation of a subscriber at
imminent risk of death during exigent circumstances threatening death or serious bodily
harm. (See, e.g., 47 U.S.C. § 222(d)(4)(A); see also 402 Michigan v. Fisher, 558 U.S. 45
(2009)).
PSAPs therefo
re may request that a carrier ping the location of an individual at imminent risk
of death or serious bodily harm when alerted to same from a crisis line. Subscriber
information can also be requested to obtain name and sometimes address or alternate
phone number.
There is no reasonably foreseeable legal risk (including with regard to HIPAA) to a PSAP for
requesting that a carrier ping the imminent risk user's location during exigent circumstances
that threaten the user's life or that of a third party. Nor is there a reasonably foreseeable legal
risk (including with regard to HIPAA) for the PSAP to provide the crisis line with disposition
information relating to the attempted rescue of such user.”
58
More inform
ation can be found in the OCR / HIPAA Privacy / Security Enforcement
Regulation Text, 45 CFR 414 164.512(j).
56
NENA 911-988 workgroup, “988 to 911 transfer draft” (unpublished manuscript, February 11, 2022).
57
NENA 911-988 workgroup. “988 to 911,” 2022.
58
National Emergency Number Association, “NENA Suicide/Crisis Line Interoperability Standard,” March 4, 2022,
https:
//cdn.ymaws.com/www.nena.org/resource/resmgr/standards/nena-sta-001.2-2022_suicide-.pdf
38

Case study: Arizona Complete Health
59
Arizona Complete Health, a provider of crisis services including a crisis line, shares
reports with system partners (e.g., PSAPs, other first responder partner agencies), which
can be tailored to specific county and time segment (
month, quarter, or year). Data is
shared bi-monthly and monthly, and organizations can request information as needed.
The items shared in the reports include:
• Crisis Line (CL) call volume and episode volume (adult and youth)
• CMT volume (adult and youth)
• CMT average response time (general calls and law enforcement calls)
• Primary Presentation–Crisis Line (adult and youth)
• Primary Presentation–CMT (adult and youth)
Information shared by PSAPs with Arizona Complete Health includes:
• BH call type volume by day of week and time of day
• Heat mapping of BH call type
• Forecasting data based on additional call type transfers
•
911 high-frequency callers identified by phone number
Systems and interoperability
The NENA Suicide / Crisis Line Interoperability S
tandard describes systems
and
interoperability principles.
Case study: The Harris Center for Mental Health and
Intellectual and Developmental Disabilities (Houston,
Texas)
60
The Harris Center integrates BH call takers alongside 911 call takers at the Houston
Office of Emergency Management from 6 am to 10 pm, seven days a week. This Crisis
Call Diversion (CCD) program is designed to decrease reliance on preventable
emergency and hospital services for people experiencing a MH crisis. Because crisis
responders sit in the Harris County 911 call center and work on the same technology
platform, they can rapidly respond to people’s needs, resulting in faster response times.
Training: At the Harris Center, BH call takers undergo rigorous training to encourage
confidence in the program and working alongside the emergency communications team.
They have a bachelor’s in psychology, sociology, or a related field. Each call taker
receives training on crisis intervention theory, cultural awareness and trauma-informed
care, rapport building and empathetic listening, privacy and confidentiality, an overview of
adult and children’s MH , substance use, and intellectual and developmental disabilities,
59
Input from Arizona Complete Health, February 2022.
60
Stephanie Hepburn, “Embedding crisis response in Harris County’s 911 dispatch center,” #CrisisTalk, December 14, 2021,
https:/
/talk.crisisnow.com/embedding-crisis-response-in-harris-countys-911-dispatch-center/; Input from Kris
tin Neylon, Project
Manager and Senior Project Associate, National Association of State Mental Health Program Directors Research Institute,
2021.
39

how to assess for suicidal and homicidal ideation, safety planning and de-escalation, and
mandatory reporting scenarios. In addition to classroom-based training, they also shadow
crisis providers: Mobile Crisis Outreach Teams (MCOTs), psychiatric ER providers, 911,
the fire department, and police department dispatchers, and even take part in ride-alongs
with officers from the police department. The training may take up to three months.
First responder diversion: Between March 2016 and March 2021, the program diverted
nearly 7,500 calls from law enforcement response, which the department estimated is
equivalent to over 11,000 police hours and more than $2 million in resources saved for
the police department. Between June 2017 and March 2021, it diverted more than 3,000
calls from fire department response, wh
ich the department estimates saved nearly $4.5
million over four years. Besides the time and resource savings the diversion program
provides the police and fire departments, the program made over 3,000 community
referrals and completed more than 2,500 safety plans with callers. Before its launch, any
calls the Harris Fire Department responded to had to be cleared by law enforcement. With
the implementation of the diversion program, counselors can sign off on MH crisis calls
without the police department, saving both agencies significant time and resources.
Enhancing the crisis continuum: In M
arch 2021, the Harris Center began a new
collaboration with the police department to automatically dispatch MH clinicians through
the Harris Center’s MCOTs. The service offers an alternative to law enforcement
response for non-violent, non-criminal 911 calls for service involving a MH issue the CCD
program could not resolve over the phone. In the four months since the project launched,
the teams have resolved 53 percent of calls they have received from the diversion
program. In addition, only 31 percent of calls for MCOT were transported to a hospital for
safety and stabilization, 13 percent required additional emergency response, and 3
percent could not be located upon arrival.
Relationships with PSAPs:
61
Harris Center PSAP partners noted, “if you’ve seen one
PSAP, you’ve seen one PSAP.” Some PSAPs have only a handful of staff while some,
like the Harris Center, have hundreds of staff. Some PSAPs are designed where the
dispatcher does everything from answer the initial call to making the dispatch and staying
on the line with the caller until a law enforcement or EMS unit arrives on scene. Other
PSAPs have each of these as specialized positions. In addition, some PSAPs use the
same dispatch teams to handle calls for service for police, fire, and ambulance while
others have multiple teams. All of these considerations make each contact with an
individual PSAP center a unique experience which will require the crisis center to be
prepared to understand the unique nature of that PSAP and how they can best benefit
from a relationship. The
Harris Center states it “is critical that a crisis center’s first
communication with their local PSAP is not to pitch the 911 / 988 collaborative.” There
needs to be some trust building and understanding about how both systems work and
interact first. People from the crisis center, the PSAP, law enforcement, and EMS all need
to be at the table to ensure all representatives’ roles are fully understood.
I
t was very important to PSAP partners to understand training and quality assurance /
performance improvement processes. It is also critical to understand the
telecommunication licensure requirements for the state if part of the plan includes co-
locating or working within computer-ai
ded dispatch-software systems.
Onc
e it has been determined that the crisis center and PSAP will work collaboratively on
calls, it is key to start with the creation of a call flow to determine under what
circumstances the PSAP will connect / transfer calls to the crisis center and what the
61
Jennifer Battle, Director of Access for The Harris Center for Mental Health and IDD Services, February 2022.
40

protocol for the crisis center is when the caller needs to be reconnected to the PSAP for
emergency response.
It is also critical to determine what sort of data needs to be collected and/or mined from
both entities so the center c
an ensure that it is seeing both the positive outcomes as well
as areas for improvement. Decis
ions about who pulls what data and when, as well as
what data can be shared across agencies, need to be di
scussed early in the written
agreement process.
Just
like crisis center new hires / vol
unteers do side-by-side shifts, there should be side-
by-side shifts at the PSAP. The PSA
P dispatchers and leaders should also be offered
side-by-sides at the crisis center. This will hel
p enhance both teams’ understanding of
work style and capability.
Case study: Didi Hirsch (Los Angeles, California)
62
Didi Hirsch’s Suicide Prevention Center (SPC) was the nation’s first and is now its largest,
fielding the NSPL, Dis
aster Distress Hotline, and local Teen Line with 24/7 bilingual
coverage of calls, chats, and text
s. The Los Angeles Police Department (LAPD) and Didi
Hirsch partnered to build a program to divert 911 calls
so those in suicidal crisis or severe
emotional distress can receive appropriate MH assi
stance. The program began for eight
hours a day and was later expanded to
a 24-hour operation.
The program was shown to lessen t
he burden on police patrol resources, decrease
violent, traumatic encounters between police and people suffering from MH crises
, and
save the local police department millions annually, with savings to healthcare and other
systems being even larger.
Building relationships with PSAPs. Didi Hirsch found that the relationship starts with local
law enforcement and
the PSAP staff. About 35 years ago, she began building these
relationships, coming in with the belief that law enforcement agencies are just as
committed to MH cr
isis de-escalation as the crisis centers. The relationship is based on
the idea that this is mutually beneficial, and that partnership can start with training. She
asked law enforcement if they could provide training to the crisis center on their response,
and also offered to provide MH de-escalation call training to law enforcement. In fact, law
enforcement representatives listened in on crisis calls and vice-versa.
As part of this bi-di
rectional learning and training, crisis counsellors and 911 operators
understood that they both experienced difficult interactions. In fact, through collaboration,
both crisis center and law enforcement team members began to understand each other at
a human level. One particularly successful element was adding crisis response training,
which included suicide prevention training, to law enforcement and PSAP standard
trainings. Didi Hirsch also identified a team member that would be a dedicated point of
contact and trainer for the local law enforcement and PSAP teams.
62
Sandri Kramer, Director of Community Relations and Special Projects, Didi Hirsch Mental Health Services, February 2022.
41

4. Additional categories
Universal and convenient access
A key tenet of 988 is “Univer
sal and Convenient Access, including omnipresent public
awareness and varying modalities for individuals to access 988 through their preferred
method of communication.”
63
This section includes informat
ion about
1. Required answer rates
2. Projections of c
ontact increases and answer speeds
3. Information about multichannel contacts (call, chat, text)
1. Required answer rates for coverage areas
Required answer rates f
or a coverage area are detailed in the table below from SAMHSA’s
Cooperative Agreements for States and Territories to Build Local 988 Capacity
(https://www.samhsa.gov/grants/grant-announcements/sm-22-015).
64
Key Performance
Indicators (KPIs)**
Definition
Target
Calls, Chats, Texts
Received
Total number of contacts
received
n/a
Calls, Chats, Texts
Answered
Total number of contacts
answered
Greater than 90 percent
Phone, Chat, Text Average
Speed to Answer**
Speed to answer contact
95 percent answered in 20
seconds, 90 percent answered in
15 seconds (network target)
Abandonment Rate
Percentage of contacts received
vs. disconnected prior to answer
Less than 5 percent
Direct / Rollover calls to
Backup centers
Total number of phone contacts
sent to the Lifeline centers
Less than 10 percent
** Select KPIs are required f
or the services (phone, chat, or text) a state or territory is
providing.
Commonly used metrics and their definitions include:
• Handle time: “the time i
t takes to take a call, including documentation time”
65
• Average speed of answer (ASA): “the amount of time it takes to answer a call (this
does not include abandoned calls)”
66
• Service level: “the proportion of calls a center answers in a certain amount of time
(out of answered calls only)”
67
63
“Vibrant and 988,” Vibrant Emotional Health, July 13, 2020, accessed February 24, 2022, https://www.vibrant.org/988/.
64
“Cooperative agreements for States and Territories to build local 988 capacity,” Substance Abuse and Mental Health Services
Administration, December 20, 2021, https://www.samhsa.gov/grants/grant-announcements/sm-22-015.
65
“Operations and Service Levels in the Lifeline/988 Network,” 2021, Vibrant Emotional Health.
66
“Operations and Service Levels in the Lifeline/988 Network,” 2021, Vibrant Emotional Health.
67
“Operations and Service Levels in the Lifeline/988 Network,” 2021, Vibrant Emotional Health.
42

Additional information: The Crisis Call Center Metrics guide
(https://suicidepreventionlifeline.org/wp-
cont
ent/uploads/2019/02/CallCenterMetrics_final.pdf).
In addition
to ensuring an opportunity to respond to all contacts, centers should maintain
focus on
the human / therapeutic connection.
68
As Vibrant writes, “With grant requirements,
it’s easy to get completely caught up in the numbers. We look at these metrics for our
planning, but do not fixate on it. There are intangibles that are the reason Lifeline exists.
What is most important is how crisis center counselors handle callers in distress. It is easy to
get caught up in call volume and cost and forget about the human connection piece. Crisis
centers are a different kind of contact center, and we have to treat them as such.”
69
2. Overvi
ew of potential expectations for increases in contacts
“In order to support the development of appropriate infrastructure and operat
ions for 988,
Vibrant has compiled models to project the populations likely to utilize 988, and the potential
volume of contacts via phone, SMS, and online chat for the first five years of 988's service”.
70
National pr
ojections can be found in 988 Serviceable Populations and Contact Volume
Projections (https://www.vibrant.org/wp-content/uploads/2020/12/Vibrant-988-Projections-
Report.pdf?_ga=2.62739180.1718066263.1611784352-1951259024.1604696443).
71
3. Approaches t
o increasing share of contacts answered and multichannel availability
(calls, texts, chats)
Resources to increase the share of cont
acts answered can be found in the
Crisi
s Call Center
Metrics (
https://suicidepreventionlifeline.org/wp-
content/uploads/2019/02/CallCenterMetrics_final.pdf).
68
James Wright, Public Health Advisor for SAMHSA.
69
“Operations and Service Levels in the Lifeline/988 Network,” 2021, Vibrant Emotional Health.
70
Vibrant Emotional Health, “988 serviceable populations,” December 2020.
71
Vibrant Emotional Health, “988 serviceable populations,” December 2020.
43

High quality and personalized experience
Another key
tenet of 988 is “High Quality and Personalized Experience that is tailored to the
unique needs of the individual while also in line with identified best practices.”
72
This section
includes information about best practices for contact center management and responding to
contacts.
According to the NSPL: “The Lifeline provides MH professionals and crisis centers in the
Lifeline network with innovative best practices
and resources in the field of suicide prevention
and M
H (https
://suicidepreventionlifeline.org/best-practices/).”
73
These best practices and
resources include:
Imminent risk
74
• Policy for Helping Callers at Imminent Risk of Suicide: Thi
s document outlines t
he
research and rationale that led to the development of the Lifeline’s polic
y for helping
callers at imminent risk of suicide. It provides a definition for what constitutes a caller
at imminent risk of suicide, informed by Lifeline’s Suicide Risk Assessment
Standards. In addition, it describes the process used to determine the core values,
definitions, and components of the policy
(https://drive.google.com/file/d/1MKdm9HC5F0LFpuLTmL0IGW0dhLZeGDT2/view)
• Checklist of Imminent Risk Requirements
: Thi
s doc
ument contains all of the required
elements of a center’s Imminent Risk Policy; it
outlines those requirements in a
checklist format
(https://drive.google.com/file/d/1aCxBfeaO4l9EJhADA21c175KKEtIKcS2/view)
• Lifeline Best Practices fo
r Helping Callers
(https://drive.google.com/file/d/1RuSEAlej-
bUB-Kt8LlFxME0qK6BniFRG/view)
Risk/safe
ty asses
sment
75
• Establishing standards for the assessment of suicide risk among callers to the NSPL:
This
document provides the background on the need for these standards, descri
bes
the process that produced them, summarizes the research and rationale supporting
the standards, and reviews how these standard assessment principles and their
subcomponents can be weighted in relation to one another so as to effectively guide
crisis counselors in their everyday assessments of callers to the Lifeline
(https://drive.google.com/file/d/1R3_wRDSN0EKjcvk9Vd3AmQ9xGfAXdggn/view)
• Suicide Risk Assessment Standards chart:
This document provides a reference chart
outlining the core principle
s and subcomponents of assessment, including the
required prompt questions
(https://drive.google.com/file/d/1F1EQ7Qvgz2wWABNYr4wyliudkHiKFATz/view)
• Risk
/ Safety Assessment Checklist:
This document contains all of the required
elements of a center’s Risk / Safe
ty Assessment and outlines those requirements in a
checklist format (https://drive.google.com/file/d/1-
roj5zbLyqXI8FnMc5cbuTsJuhWUxZ8X/view)
72
“Vibrant and 988,” July 13, 2020.
73
“Best practices,” National Suicide Prevention Lifeline, accessed February 26, 2022, https://suicidepreventionlifeline.org/best-
practices/.
74
National Suicide Prevention Lifeline, “Lifeline best practices and clinical resources,” updated November 2020,
https://988vibrant.grant.org.
75
National Suicide Prevention Lifeline, “Lifeline best practices and clinical resources,” 2020.
44

Other policies, documents, and training required in network agreements
76
• Network Agreement Provision of Resource Referrals requirement
(https://docs.google.com/document/d/1fbJW-jzi1KZnNZv3X-
eOZ0CjinMbOg2K8WAAdsN58hc/edit)
• Network Agreement Grievance / Complaint / Caller Action requirements
(https://docs.google.com/document/d/136omXR96zIO0OPuVFoXOZG8p-
FDzO9ohhjNWiKQbYDg/edit)
• Network Agreement Training requirements
(https://docs.google.com/document/d/1KFTemyGfvx2AaxlujqfTiab-
vg5vgF4XxfaDTq2WUD8/edit)
Info
rmation on related and additional topics can be found in the Practice Guidelines section
of the NRC
, inc
luding :
URL:
(ht
tps://networkresourcecenter.org/plugins/servlet/samlsso?redirectTo=%2Fpages%2Fviewp
age.action%3FspaceKey%3Dpracticeguide%26title%3DTip%2BSheets)
• “Contact center management: This page contains best practice guidelines for
managing a contact center
• Follow-up: Follow-up has become an integral part of crisis center services. This page
provides a wealth of information on providing follow-up services to both Lifeline
callers and those recently discharged from inpatient or emergency department
settings
• Good contact: This page contains information on good contacts and collaborative
problem-solving
• Imminent risk: The Lifeline policy for helping callers at imminent risk of suicide was
adopted throughout the network in 2012. Detailed information on this policy is
included here as well as information on how to ensure center policies meet this
network requirement. Crisis center examples of approved policies are provided
• Lifeline crisis chat / text: The Lifeline Crisis Chat (LCC) program was officially
launched in February 2013. Information is provided on the value of chat service
provision and the steps to take to join the LCC Network
• Postvention: This page contains information on postvention as well as supporting
documentation
• Quality practice: In January 2014, the Lifeline distributed the best practices for
helping callers to the Lifeline network of crisis centers. This page provides information
on the development of this document and links to supporting documentation and
resources to assist with quality programming
• Safety assessment: This page contains information on the Lifeline Safety
Assessment as well as supporting documentation
• Safety planning: This page provides information on safety planning and links to
training resources for safety plan development
• Violence / threat management: This page contains information about the violence
assessment and threat management webinar series with links to the recordings and
handouts as well as supporting documents with recent research and resources for
those with further interest in the topics.”
77
Tip sheet
s for specialized interventions can also be found in the NRC
, i
ncluding on inclusive
language, LGBTQ youth guidelines, maternal MH ,
psychotic symptoms, gambling disorders,
working with American Indians / Alaska Natives, working with the deaf community, and
76
National Suicide Prevention Lifeline, “Lifeline best practices and clinical resources,” 2020.
77
“Practice guidelines,” Lifeline Network Resource Center, n.d.,
https://networkresourcecenter.org/plugins/servlet/samlsso?redirectTo=%2Fpages%2Fviewpage.action%3FspaceKey%3Dprac
ticeguide%26title%3DFollow-Up.
45

working with individuals with substance use concerns, among many others
(https://networkresourcecenter.org/plugins/servlet/samlsso?redirectTo=%2Fpages%2Fviewp
age.action%3FspaceKey%3Dpracticeguide%26title%3DTip%2BSheets).
Connection to local resources and follow-up
Another key tenet of
988 is “connection to resources and follow-up to ensure all persons
contacting 988 receive additional local community resources as needed.”
78
Follow-up
“Cris
is centers are uniquely positioned to be a crucial resource for people in need of follow-
up care and are a vital resource for linking patients to services and providing emotional
support.”
79
Most centers provide “some form of follow-up service. Programs ranged from
follow-up services for familiar callers, monthly check-ins for high-risk callers, ED / inpatient
discharges, high-risk callers, and third-party calls.”
80
Resources for follow-up car
e: SAMHSA has made significant investments to ensure follow-
up care is integrated within crisis centers within the Lifeline. Funding opportunities for
initiatives such as follow-up care can be found on SAMHSA’s website
, when / if listed
(https://www.samhsa.gov/gran
ts).
81
SAMHSA has p
rovided direct grant funding to expand follow-up services through the
Lifeline’s contact centers. This program was intended to create an integrated hub that: “(1)
ensures systematic follow-up of suicidal persons who contact a NSPL Crisis Center; (2)
provides enhanced coordination of crisis stabilization, crisis respite, and hospital emergency
department services; and (3) enhances coordination with mobile on-site crisis response. In
effect, with the resources provided, the hub should not lose track of a person in a suicidal
crisis as they interface with crisis systems.”
82
The goal is to ensure “continuity of care to
safeguard the well-being of individuals who are at risk of suicide.”
83
Additional in
formation:
About follow-up care and effectiveness: In 2016, the Lifeline created the
Follow-Up Matters
microsite
(https://followupmatters.suicidepreventionlifeline.org/?_ga=2.34605221.544625352.1646010
686-1989988634.1643164991) as a resource for contact centers, emergency departments,
and other providers and stakeholders who are interested in creating and supporting follow-up
partnerships. The microsite provides resources such as information on getting started with
follow-up partnerships, access to research and statistics that support follow-up initiatives,
78
“Vibrant and 988,” July 13, 2020.
79
“Follow-up,” Lifeline Network Resource Center, n.d.,
https://networkresourcecenter.org/plugins/servlet/samlsso?redirectTo=%2Fpages%2Fviewpage.action%3FspaceKey%3Dprac
ticeguide%26title%3DFollow-Up.
80
“Follow-up,” Lifeline Network Resource Center.
81
“Grants,” Substance Abuse and Mental Health Services Administration, https://www.samhsa.gov/grants.
82
Note: “Eligibility is limited to NSPL Crisis Centers because they have been specifically trained in NSPL procedures pertaining
to follow-up of persons at imminent risk of suicide and in risk assessment and are the only entities that can obtain the required
consents from NSPL Crisis Center callers for follow-up activities. This eligibility limitation ensures that the infrastructure is in
place to serve high-risk, high-priority, and/or underserved populations. Limiting eligibility also ensures that relationships with
local and state mental health systems are in place for NSPL Crisis Center callers, and that individuals discharged from
partnering agencies receive follow-up care and access to treatment.” Source: “Suicide prevention lifeline crisis center follow-up
expansion grant program,” Substance Abuse and Mental Health Services Administration, January 9, 2019,
https://www.samhsa.gov/grants/grant-announcements/sm-19-008.
83
“Suicide prevention lifeline,” 2019.
46

tools for use in assessment and follow-up, sample materials, examples and profiles of
current follow-up partnerships under the current SAMHSA Follow-up grant, and more.”
84
Guidance for
follow-up care: This can be found on the NRC’s Follow Up
(https://networkresourcecenter.org/plugins/servlet/samlsso?redirectTo=%2Fpages%2Fviewp
age.action%3FspaceKey%3Dpracticeguide%26title%3DFollow-Up) page.
Collaborat
ing with peer support / warmlines
“Peer support services are profoundly valuable and fill an important role in the continuum of
care that supports individuals seeking crisis services. The Lifeline also fills an important and
different role in that continuum of care. Callers having the option and ability to choose the
type of support they feel works best for them, which is important when different modalities for
support exist in the individual’s area.”
85
“A warm l
ine is an alternative to a crisis line that is run by ‘peers,’ generally those who have
had their own experiences of trauma that they are willing to speak of and acknowledge. Most
warm line operators have been through extreme challenges themselves and are there
primarily to listen. A warm line has the purpose of reducing hospitalization and forced
treatment, being a cost effective and non-intrusive, voluntary intervention.”
86
Additional
information: How the Lifeline centers collaborate with peer support / warmlines
is available in the NRC
. Multiple organizations have lists of warmlines that they try to keep as
up-to-date as possible:
• War
mline.org’s Dire
ctory
(h
ttps://warmline.org/warmdir.html)
• Mental Health America’s (MHA’s) lis
t of available warmlines
(https://screening.mhanational.org/content/need-talk-someone-warmlines/)
• NAMI’s National W
armline Directory (https://nami.org/NAMI/media/NAMI-
Media/Helpline/NAMI-Na
tional-HelpLine-WarmLine-Directory.pdf) and the NAMI
HelpLine
(an information and resource referral helpline that can connect help seekers
with NAMI programs, NAMI support groups, and peer-inf
ormed national resources—
https://www.nami.org/help)
Relationships w
ith in-person care sites
To build a strong continuum of care, centers and in-person sites of care can establish
linkages to other sites of care, including mobile crisis services, CSRFs, peer-run respites,
and emergency departments.
8788
Mobi
le crisis services, e.g., MCTs:
89
Connecting individuals in crisis to mobile crisis
services, as appropriate, is an essential element of an integrated crisis system. Examples of
MCTs in three communities can be found in the TAC report on Mobile Crisis Teams: A State
planning gui
de for Medicaid-financed crisis response services
84
“Follow-up,” Lifeline Network Resource Center.
85
“Collaborating with peer support / warmlines,” Lifeline Network Resource Center,
https://networkresourcecenter.org/plugins/servlet/samlsso?redirectTo=%2Fpages%2Fviewpage.action%3FspaceKey%3Dprac
ticeguide%26title%3DTip%2BSheets.
86
Daniel Fisher, President, National Coalition for Mental Health Recovery.
87
SAMHSA. 2020. ”National guidelines for behavioral health crisis care – best practice toolkit,” Substance Abuse and Mental
Health Services Administration, pg. 25, 2020, https://www.samhsa.gov/sites/default/files/national-guidel
ines-for-behavioral-
health-crisis-care-02242020.pdf.
88
Daniel B. Fisher et al., “Peer-run respites: An effective crisis alternative,” Substance Abuse and Mental Health Services
Administration, n.d., https://www.nasmhpd.org/sites/default/files/Peer%20Run%20Respite%20slides.revised.pdf.
89
Jordan Gulley et al., “Mobile crisis teams: A State planning guide for Medicaid-financed crisis response services,” Technical
Assistance Cooperative and California Health Care Foundation, January 2022, https://www.tacinc.org/resource/state-planning
-
guide-for-medicaid-financed-mobile-crisis-response/.
47

(https://www.tacinc.org/resource/state-planning-guide-for-medicaid-financed-mobile-crisis-
response/).
90
Crisis
receiving and stabilization facilities (CSRFs):
91
CSRFs can take many forms; in
many communities, CCBHCs provide access to these services. CCBHCs are involved across
the crisis continuum, with prevention, crisis response (24/7 mobile teams, crisis stabilization,
suicide prevention), detoxification, coordination with law enforcement and hospitals, and
post-crisis care. 100 percent of CCBHCs provide crisis support and many operate crisis call
lines.
To find nearby CCBHCs, visit the CCBHC Success Center
or emai
l
.
92
The chart bel
ow from the National Council for Mental Wellbeing describes some of the
different names used for facility-based care.
93
Peer-run r
espites:
94
Peer-run respites are another model of short-term facility-based care. A
peer respite is a voluntary, short-term, overnight program that provides community-based,
non-clinical crisis support to help people find new understanding and ways to move forward.
It operates 24 hours per day in a homelike environment. As of March 2021, peer respites are
currently operating in California, Florida, Georgia, Iowa, Massachusetts, Nebraska, New
Hampshire, New Jersey, New York, Ohio, Pennsylvania, Vermont, and Wisconsin. Peer
respites are staffed and operated by people with psychiatric histories or who have
experienced trauma and/or extreme states. This means that: 1) 100 percent of staff have
lived experience of extreme states and/or the BH system; 2) All individuals in program /
house management positions have lived experience of extreme states and/or the MH
system; 3) Job descriptions for program / house management positions require lived
experience of extreme states and/or the MH system; and 4) The peer respite is either
90
Gulley, “Mobile crisis teams,” 2022.
91
“Crisis care continuum integration: Crisis stabilization units and in-patient psychiatric units,” June 16, 2021, Vibrant Emotional
Health
92
Rebecca Farley David, “CCBHC and 911 / PSAP partnerships: Building comprehensive referral resources and strategies,”
Vibrant Emotional Health and Education Development Council,
93
“Crisis care continuum integration: Crisis stabilization units and in-patient psychiatric units,” June 16, 2021, Vibrant Emotional
Health
94
Daniel Fisher, President, National Coalition for Mental Health Recovery.
48

operated by a peer-run organization OR has an advisory group with 51 percent or more
members having lived experience of extreme states and/or the BH system.
The National Empowerment Center (NEC) compiles a directory of peer respites
(https://www.peerrespite.com/directory/).
95
Emergency departments: Examples of different types of partnerships that contact centers
have developed with Emergency Departments, as well as strategies of how to go about
creating these relationships, can be found in the Emergency Department Partnership Toolkit
(https://networkresourcecenter.org/plugins/servlet/samlsso?redirectTo=%2Fdownload%2Fatt
achments%2F8421462%2FLifeline%2520Crisis%2520Center-
Emergency%2520Department%2520Partnership%2520Toolkit.pdf%3Fversion%3D1%26mo
dificationDate%3D1536862438957%26api%3Dv2).
95
“Peer respite directory,” last updated 2018, https://www.peerrespite.com/directory/.
49
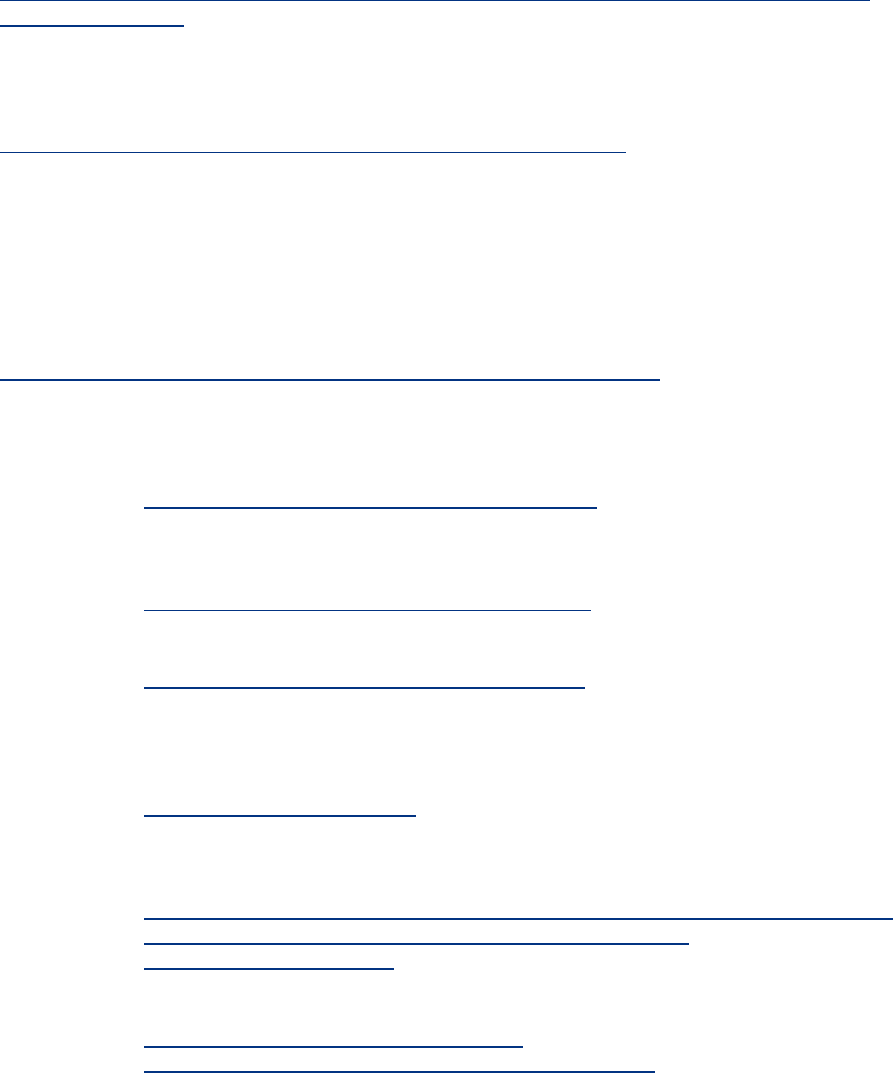
III. Additional resources
Compiled below are additional resources for Lifeline contact centers:
Substance Abuse and Mental Health Services Administration (SAMHSA)
National Guidelines for Behavioral Health Crisis Care
https://www.samhsa.gov/sites/default/files/national-guidelines-for-behavi
oral-health-crisis-
care-02242020.pdf
Crisis care best practice toolkit
Substance Abuse and Mental Health Services Administration (SAMHSA)
988: America’s Suicide Prevention and Mental Health Crisis Lifeline
https://www.samhsa.gov/find-help/suicide-prevention/988-lifeline
Preparing for 988, Frequently asked questions (FAQ)
Substance Abuse and Mental Health Services Administration (SAMHSA)
Crisis services for Child, Youth, and Family Guidelines
Forthcoming
Centers for Disease Control and Prevention (CDC)
Health Equity Guiding Principles for Inclusive Communication
https://www.cdc.gov/healthcommunication/Health_Equity_Lens.html
Inclusive communication principles
Lifeline Network Resource Center (NCR)
• Call Specialist Resources
o https://networkresourcecenter.org/category/csr
o Information about in-call tools, practice guidelines, specific populations,
training, enrichment, and research and evaluation
• Center Operations R
esources
o https://networkresourcecenter.org/category/co
o Information on data, media, 988, sustainability, funding, and zero suicide
• Lifeline Operations R
esources
o https://networkresourcecenter.org/category/lo
o Information on committees, network information, partnerships, and policy
Vibrant Emotional Health / National Suicide Prevention Lifeline
• Vibrant and 988
o https://www.vibrant.org/988/
o Frequently asked questions (FAQ), documents for stakeholders, Vibrant
statements on 988, press releases and statements
• 988 Serviceable Populations and Contact Volume Projections
o https://www.vibrant.org/wp-c
ontent/uploads/2020/12/Vibrant-988-Projections-
Report.
pdf?_ga=2.62739180.1718066263.1611784352-
1951259024.1604696443
o Projected contact volume
• Crisis Call Center Metrics
o https://suicidepreventionlifeline.org/wp-
c
ontent/upl
oads/2019/02/CallCenterMetrics_final.pdf
50
Note:
In addition to the sources noted above, this document incorporates information shared during
the Lifeline Contact Centers Working Group meetings of partners of the SAMHSA /
NASMHPD 988 co-sponsorship (December 2021 – March 2022).
51

IV. Appendix
Appendix A: Active surge management example protocol
from BHR
Example prot
ocol
96
• If calls hold for two minutes:
o An automated email notification will go out to all of the on-call
management
team
o If the Operations Analyst is available, they will notify the contact center leads
and manager
s that they are taking care of notifying CICs who need to get i
n
queue v
ia email and/or teams to individual/s
The Operations Analyst will also note any DND and call lasting longer
than 10 minutes during the surge
A clinical staff member who supports the contact center leads and
a
m
anager (
the person with the most seniority, who is on shift first)
will
s
tay out of queue to assist CICs by taking over their Telehealth /
Mobile outreach team (MOT) dispatching and staffing during the surge
o If Operations Analyst is not available, the st
aff with the most seniority, who is
on shift first, will monitor the dashboard for calls waiting and will also stay out
of the queue to assist with all staffing needed during the surge. They will k
eep
t
he dashboard and teams open on their scr
een
• At
two minutes, con
tact center staff who are not on lunch, break, actively working with
IT, or in a scheduled meeting with their supervisor must beco
me available
o If sending a MOT, telehealth, or on-call email, leads and managers and the
per
son with the most seniority (as noted above) will do it. Leads will sto
p
m
aking outbound SL calls at this mark
• At four minutes, al
l clinical staff need to log in (i.e., leads, CCC, managers) except for
one
identified person (as noted above) who handles staffing, contacting MOTs /
Telehealth / or on-call resources
Ongoing S
urge / Extended Surge
• Notice of emergency call coverage: Contact the Operat
ions Analyst and the Clinical
Director of the contact center
• If high surge volume continues, at
30 minutes maximum or earlier based on the
manager
s / leads discretion, the Clinical Director will be contacted about the iss
ue
• I
f the Clinical Director does not believe this will be resolved in less than an hour,
they
will contact the Chief Clinical Officer
96
Behavioral Health Response via National Council for Mental Wellbeing.
52

Appendix B: MOUs between contact centers and PSAPs
E
xample A – Simple MOU: between XYZ Crisis Center and ABC County 911 Services
97
Thi
s Memorandum of Understanding (MOU) outlines the working relationship between XYZ
Crisis Center and the ABC County 911 System.
• Insert paragraph detailing programs and services of ABC County 911
• Insert paragraph detailing programs and services of XYZ Crisis Center
The f
ollowing information is provided to both parties for coordination purposes:
Responsibilities of the XYZ Crisis Center under this MOU:
• XYZ Center crisis counselors will accept calls referred by 911 operators from callers
seeking non-emergent help with suicidal thoughts or emotional crises
• XYZ Center crisis counselors will instruct callers needing emergency services, such
as fire, law enforcement, or medical services, to hang up and dial 911
• XYZ Center crisis counselors will attempt to collect appropriate information from
callers unable or unwilling to dial 911 and transmit that information to the appropriate
911 PSAP (Public Safety Answering Point)
• XYZ Center crisis counselors will, when a caller or chat visitor is determined to be at
imminent risk for suicide / suicide in progress, collect as much information as possible
on the circumstances and notify the appropriate PSAP. This will include information
on the suicide plan, potential weapons, and other known dangers to responding
emergency personnel. The XYZ crisis counselor will remain on the line with the caller
as long as possible. In these circumstances, the crisis counselor will share any caller
ID information, address / location, IP address, or any other identifying information the
caller has shared
Responsibilities of the ABC County 911 System under this MOU:
• ABC County 911 Operators will, at their discretion, refer or transfer callers in
emotional crises to the XYZ Crisis Center. When possible, 911 Operators will inform
crisis counselors that they have transferred a call and let the crisis counselor know
whether they intend to monitor the call
• ABC County 911 Operators will use the identifying information provided by the crisis
center for situations involving imminent risk of harm / harm in progress and assist with
location and dispatch of emergency services to these callers / chat visitors 24 hours
per day when requested by the XYZ Crisis Center
• This MOU shall take effect upon the date signed by both parties and shall be
reviewed annually. Either party shall be allowed to terminate this MOU by submitting
a written letter to the other party.
X
YZ Crisis Center Name / title, Signature & Date
ABC County 911 Name / title, Signature & Date
97
Input from Vibrant Emotional Health, 2022
53

Example B – MOU centers that are blended crisis / information and referral lines:
98
M
emorandum of Understanding between blended crisis center and sample PSAP
Center Name is a non-profit organization in City, State that answers various hotlines
including xxx and xxx, and local area calls for the NSPL. The hotlines provide callers with
24-hour telephone crisis / suicide prevention and community information and referrals.
Purpose:
This memorandum describes and documents the working relationship between Center
Name and the PSAP Name (hereafter referred to as 911) in order to enhance delivery of
Information & Referral, Crisis Intervention, and Suicide Prevention services to community
residents and assist with the non-emergency calls to 911.
Center Name and other local nonprofits, community organizations, and government
agencies share a common mission of serving their communities. They seek to improve
access to community health and human services and to serve as community barometers to
indicate insufficient resources and gaps in services. With that mission in mind, Center Name
is proud to partner with 911 to provide the community with appropriate information and
referral, crisis intervention, and suicide prevention services and to limit non-emergency calls
to 911.
Each party to this memorandum is a separate and independent organization and nothing
herein shall be constructed to create a joint venture or legal partnership. Each organization
shall retain its own identity in providing services.
Center Name and 911
agree to the following:
C
omponent I: Confidentiality
1. Client confidentiality is to be maintained by Center Name s
taff and volunteers at all
times, except when the client gives the crisis counselor explicit verbal permission to
share specific information with an agreed-upon entity for purposes of advocacy / referral
or in cases where the crisis counselor learns of imminent danger to a person or persons,
or in cases where the crisis counselor learns of abuse or neglect of a minor, disabled
adult, or elder.
2. Every person contacting Center Name has the right to receive services without divulging
his/her identity. Services provided to a client should in no way be affected by their choice
to maintain anonymity. However, certain demographic and other information is requested
and recorded for purposes of maintaining confidential client records and aggregated call
reports.
3. Center Name and
911 will comply with all applicable federal, state, and local
confidentiality laws.
4. Center Name will p
rovide 911 with an aggregated data report of contacts referred to the
911 on a quarterly basis.
5. Center Name crisis counselors will consult with a supervisor prior to breaching a
contact’s confidentiality, except with suicide in progress contacts, violence in progress
contacts, or contacts where the person has become unconscious.
98
Input from Vibrant Emotional Health, 2022
54
Component II: Community Collaboration
1. Center Name and 911 will communicate, at least annually, to evaluate mutual processes
and practices and make changes to this memorandum of agreement as needed.
C
omponent III: Client Contacts
1. 911 may direct callers requesting non-emergency related information and referral
services to Center Name through referral, call transfer, or call conferencing processes.
2. 911 may direct callers in crisis or those individuals wanting to speak with a crisis
counselor and not have Emergency Medical Services (EMS) respond to their location to
Center Name through referral or call transfer or call conferencing processes.
3. 911 may call conference Center Name for callers in crisis who have EMS responding to
their current location.
4. Center Name crisis counselors will consult with a supervisor prior to calling 911 for
callers who require emergency services due to imminent risk for suicide or violence.
5. Center Name can provide a presentation to 911 staff, as requested by 911 and the
schedule availability of Center Name.
C
omponent VI: Termination
Shall either Center Name or 911 decide to terminate this memorandum of agreement they
shall send written notice of intent to the other party 30 days prior to termination, which shall
conclude all activity detailed in this agreement. Each party shall remove references to this
agreement from their website and other similar documents.
For Center Name.:
Center Representative Name / Title
For PSAP Name
PSAP Representative Name / Title
55

Appendix C: LAPD 911 dispatch protocol for diverting calls
involving persons experiencing a mental health crisis to
Didi Hirsch
99
The f
ollowing situations shall be considered for transfer to Didi Hirsch:
• Suicide attempt or suicidal thoughts
• Possible suicide attempt or suicidal thoughts
• Mental illness
• Possible mental illness
The oper
ator r
eceiving the call shall conduct a thorough interview and determine if the
circumstances meet any of the following criteria:
• The caller is threatening to jump from a bridge or structure
• The caller needs medical attention
• A suicide attempt is in progress
• The caller has a weapon and is in public with others present
• The caller has a weapon, is inside a residence / b
uilding, and with others present
If any o
f the above criteria are met, the operator shall follow established policies, procedures,
and guidelines and dispatch a patrol unit / SMART and/or transfer to the Los Angeles Fire
Department (LAFD).
If none of the above criteria are met, the operator shall:
1. Create an incident in the PremierOne Computer Aided Dispatch system and
at
tempt to obtain the caller’s name, location, phone number, and any pertinent
information. The incident shall be closed using the “CTR” disposition code and
“transferred PR to Didi Hirsch” noted in the comments.
Not
e: If the caller refuses to provide their location, the operator shall use the
address of the Metropolitan or Valley Communications Dispatch Center.
Location information provided by Automatic Location Information and/or
RapidSOS shall be entered into the comments of the incident in the event it is
needed later.
2. Advise the caller they are being connected to a crisis counselor and not to hang
up.
Tell the caller you are going to provide the counselor with some background
information while the caller is on the line.
Exam
ple: “I am going to connect you with a crisis counselor that can help
you, please don’t hang up. When the counselor answers, you are going to
hear me give them some background information on you and what you’re
experiencing today. After that, you will remain connected to the counselor, and
I will drop off the line.”
3. Conference the caller with Didi Hirsch using the dedicated phone number (424)
xxx
-xxxx. This number is programmed into the Power 911 application in the “Quick
Dial” section. Searching the key words “mental” or “suicide” will also display the Quick
Dial entry.
99
Sandri Kramer, Suicide Prevention Program Director at Didi Hirsch Mental Services.
56
4. Announce to the counselor that you are from LAPD and have a caller on the line,
introduce the caller by name, and provide a brief synopsis of the situation.
Example: “This is Operator 123 from LAPD. I have James on the line, and
he’s been depressed recently over the death of his spouse. He reached out
for some help today.”
5. Provide the counselor with the incident number, caller’s address, phone number,
and any other pertinent information.
6. Indicate that you are dropping off the line then release the call.
57

Appendix D: LAPD 911 diversion guide for crisis
counselors and supervisors
100
How will I know it is an LAPD 911 Diversion call?
• Starting Feb. 1, you will see an additional queue / phone l
ine called “LAPD 911
Diversion” added onto our system
• Staff and volunteers who have completed the apprenti
ceship will be the only ones
who can see and receive calls from this line
• This line will not roll and must be answered (has been programmed as a priority line
above all ot
her lines)
• ‘LAPD 911 Diversion’ will also auto-populate i
nto the iCarol report under ‘Line Called’
What types of
transfer calls we will receive:
• Calls transferred to us will be those in emotional distress, MH cris
is, or suicidal crisis
**For exact criteria, please see LAPD Dispatch Protocol for 911 Diversion**
• Calls on this line will only be from LAPD 911 Dispatch, not CHP operators or other
entit
ies. Other law enforcement agencies may continue to cold or warm transfer calls
to us on our other lines as they always have
• LAPD should not divert crime-rel
ated calls to us nor calls where a person is already in
imminent danger or physically harmed and needs immediate medical attention
• Our role as crisis line counselors remains the same and we are expected to continue
util
izing our crisis-line training to handle these calls. It is not expected for us to have
any specialized training for this service. The diverted calls are from people who
should have called us to begin with, not 911. Please handle all calls as you normally
would on any of our lines
• If you receive calls outside of these parameters, please still take the call:
o After the call, please notify your supervisor
o Supervisors: Please add the call report in the on-call email and note this
All call
s from LAPD 911 Diversion should be warm transfers (i.e., the LAPD 911 operator
will provide you with information with the caller still on the line)
• If any call is cold transferred (you are immediately connected to the caller without
being handed off
by the operator first), please inform your supervisor
• Supervisors: Please add this to the call report and note what happened in the on-call
em
ail
You should receive the following information from the Operator:
• Caller’s name
• Caller’s phone number
• Caller’s address or location (if exact address is not available)
• Reason for the transfer
• Incident number
• Operator Number
• It is okay to ask background questions of the operator to ensure you get important
i
nformation
How
to handle the call with the caller
• Start from the beginning like a regular call, do not assume all information from the
oper
ator is correct but use it as a prompt to start the interaction
100
Sandri Kramer, Suicide Prevention Program Director at Didi Hirsch Mental Services.
58
• Continue using your crisis line training to take the call as you would any call on the
lines
• ALWAYS OFFE
R A FOLLOW-UP CALL to the caller, regardless of presence or level
of suicidality / risk. This is a mandated part of our contract with LAPD 911 Dispatch
o The only exception is if the caller is abusive. Please document why a follow up
w
as not offered when this occurs
o Depending on the risk of the caller, you can decide if a high risk or standard
f
ollow-up is needed
o You will document the reason for follow-up as
‘Contracted Follow-Up Service
(911 Diversion, ELAC, EDFU). This check box has been added to the call
report
If
the call turns into a rescue and emergency services are needed:
• SUPERVISORS ONLY: C
ALL OUR LAPD DISPATCH SPECIFIC NUMBER:
(xxx)xxx-xxxx and provide the incident number to let them know a rescue is needed
o COUNSELOR WILL NOT TRANSFER CALLER BA
CK TO 911
The only exception would be if caller explicitly requests to be
t
ransferred back and the supervisor deems this to be appropriate
o Dispatch will know who the caller is based on the incident number
• This Dispatch Specific Number is to be used by supervisors mainly for 911 Diversion
callers needing rescue
o Supervisors CAN also us
e this direct line for callers needing rescue from other
lines if they are confirmed to be located within the Los Angeles city area
• This is considered a rescue and should be t
reated as any other rescue (counselor will
stay on the line with caller while supervisor contacts dispatch and until emergency
rescue arrives)
59
